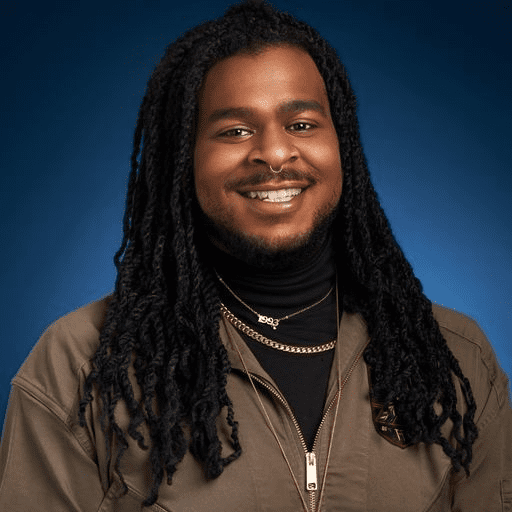
Terry Dudley is a Black queer Southsider who has dedicated their life to HIV activism since they first accessed LGBTQ+ resources after coming out to a healthcare provider at 16 years old. “My first experience with a youth space was on the Northside being escorted through back doors, being told you can't use the main entrance in the name of your own safety,” said Terry. Feeling excluded in healthcare settings has not been an isolated experience for Terry as they continued to be involved in these spaces personally and professionally.
One focus of Terry’s work is youth capacity building; they help with curriculum building through Chicago Public Schools and different youth programs to ensure young people feel included in their own healthcare. “What has been the most fulfilling is when I get an opportunity to work with young people and talk to young people about what they can do to help prevent HIV, and how to even talk about it and feel more affirmed in it,” said Terry.
Alongside their work with youth, Terry is a health educator, HIV screener, and community organizer participating in projects such as HIV and The Journey Toward Zero, raising awareness about the disproportionate impact of HIV on people of color.
Part of what drives the disproportionate impact of HIV on Black and Latinx communities is systemic racism and white supremacy culture. Specifically, Terry studies spatial stigma, the idea that a racially biased stigma is attached to a place that then dictates the scope of resources and services that that place will receive. “The stigma attached to the Southside is ‘you should just be grateful that we are here, and if you need anything more than an HIV test, you need to go up North because that's where the real services are,’” said Terry.
“It is how we tell Black and brown people that your neighborhoods aren't good enough for these resources or when we do put these resources in there it is because we want to redevelop those neighborhoods.”
Where we invest our resources says a lot about who we care to invest in. Through working in clinics for many years, Terry has seen firsthand the different types of treatment people receive based on the color of their skin and the type of resources available on the Northside compared to the Southside of Chicago.
Terry recalls a client entering a clinic setting who was experiencing a serious mental health episode. “If they are Black, they are met with extreme aggression,” said Terry. “I am seeing in the chat amongst the faculty and staff that this person is being aggressive, we need the safety team in here vs. I've seen it in the same space where if we have a white client who is living in a different reality, then we are calling a psychiatrist and we are also calling a therapist to come meet the client.”
There are also differences in responses based on location because of the stigma attached to certain spaces. “Responses like that just don't happen on the Southside because if you are coming in escalated, you won’t receive any services,” said Terry. Working at Southside clinics, Terry has had clients coming in who are upset; if they get too loud or start yelling, they can be escorted out of the clinic and banned from these spaces, now losing access to any services.
“I know what it's like being 15 and having to go up North – I know the safety issues that I encountered a lot of times, and it's just worrying,” said Terry.
In 2021, Black people made up 51.8% of people newly diagnosed with HIV in Chicago, despite making up 32.5% of Chicago’s population (aidsvu.org). With the majority of Black people living on the Southside, Terry notes that HIV resources and clinics are mainly still centered on the Northside of Chicago. “That says a lot to me, as someone who has been experiencing these spaces for the last 15 years, to see that there has still been nobody to break the ground on the Southside and be intentional with it,” said Terry. “Agencies will go and have an event on the Southside but won't build their office brick and mortar on the South or West sides.”
Access to healthcare – and culturally competent care – should not be a privilege. In Chicago, young people aged 13-19 have the lowest rate of viral suppression* (40%) of all age groups, followed by people aged 20-29 (56%); youth living with HIV are disproportionately Black and are less likely to be successfully treated for HIV (GTZ IL, 2021). Without access to clinics in their neighborhoods or robust support systems, young Black people are less likely to be engaged in care let alone stay in care, Terry says.
“It is easier to say it but harder to do it and you already have Black people in the community who feel disinvested so I worry because I know what that would do – having a dedicated youth space on the Southside.”
For agencies and nonprofits working toward ending the HIV epidemic, declaring racism a public health crisis and responding as such is crucial. Beyond that, Terry wants to see agencies truly value lived experiences. “There are a lot of Black and brown people who do this work and do it at an entry level sometimes for 20 years testing people but would never be a manager or director in an agency because they did not get their degree because in their youth, they were just trying to survive and help their communities,” said Terry.
“I hit the ceiling in nonprofits where I was trying to be an HIV manager and lead a team, and I was told that because I did not have a degree, I would not move past mid-management.”
Often due to systemic racism, Black people don’t have the same access to education and other opportunities compared to their white counterparts but have still been gaining experiences and knowledge working first-hand in the communities they are trying to serve.
“What I've seen in HIV work, it is usually built on the backs of people demanding the idea that our lives matter, we deserve the same treatment and care, and we don't always get it,” said Terry.
To close health disparities and respond to racism as a public health crisis, agencies including AIDS Foundation Chicago must be willing to adjust their practices and processes to allow for the people most affected by HIV to be at the forefront of our work and be the ones driving the solutions.
“Before I came into this world, I had no choice of who I would be,” said Terry. “As a Black person, I am at higher risk for medical malpractice, higher risk for being murdered by authority figures, higher risk of incarceration – if you take my blackness out of my skin, all those risks go away. It doesn't mean those risks wouldn't exist for me, it's just that the rates go down astronomically.”
“I can't hide being Black; I am always going to be a large 6’2 Black person that is imposing to someone who isn't my body type and size and who has been taught that large Black people will harm you,” said Terry.
To help AFC dismantle racist healthcare systems and take action for health policy, join our mobile action network.
*Viral suppression supports one’s individual and community health, as someone who is virally suppressed is healthier and cannot pass HIV sexually to their partners – this is known as U = U, or Undetectable = Untransmittable.