The AIDS Foundation of Chicago (AFC) is gravely disheartened to learn about the Trump Administration’s plans to redirect $266 million earmarked for social services pay for the detention of children separated from their families at the U.S.-Mexico border. The funding includes $9.5 million for HIV programs.
While the Trump administration has the authority to transfer funds among programs, we strongly oppose any diversion of Ryan White HIV/AIDS Program and HIV prevention funds for purposes not related to caring for the 1.2 million people living with HIV in this country, or preventing new cases of HIV. We are especially opposed to using funds intended to support health goals for people to cover the cost of a cruel and inhumane policy like the child separation border policy.
It is our understanding that the list of planned transfers below are all from the current fiscal year (FY 18) and are from unobligated or unspent funds.
- $5.75M from ADAP in Ryan White (HRSA)
- $1.2M from HIV Prevention by Health Departments (CDC)
- $1.4M from HIV Surveillance (CDC)
- $138K from Viral Hepatitis (CDC)
- $558K from STIs (CDC)
- $504K from TB (CDC)
- $436K from Global HIV (CDC)
- $12.1M from NIAID (NIH) – unclear whether HIV specific
- $131K from SMAIF (Office of the Secretary)
- $1.036M from MAI (SAMHSA)
- $5.3M from Substance Abuse Screening, Brief Intervention, and Referral to Treatment (SAMHSA)
Other accounts being raided include the National Cancer Institute, Head Start, runaway and homeless youth programs, funds for violent crime reduction in women’s shelters, maternal and child health block grants, and more.
AFC insists that any unspent Ryan White or HIV prevention funding is redirected towards HIV programs and services. We strongly condemn the use of HIV funding — unspent or otherwise — to support the Trump Administration’s xenophobic practice of child separation that has resulted in trauma to immigrant children and families. At a time when more funding is needed to end the HIV epidemic, it is unwise to divert funding to this inhumane program. AFC will continue to work with our partners to monitor and oppose this policy. In the meantime, join us in expressing your outrage of this inhumane policy by taking action using this action alert sponsored by AIDS United.
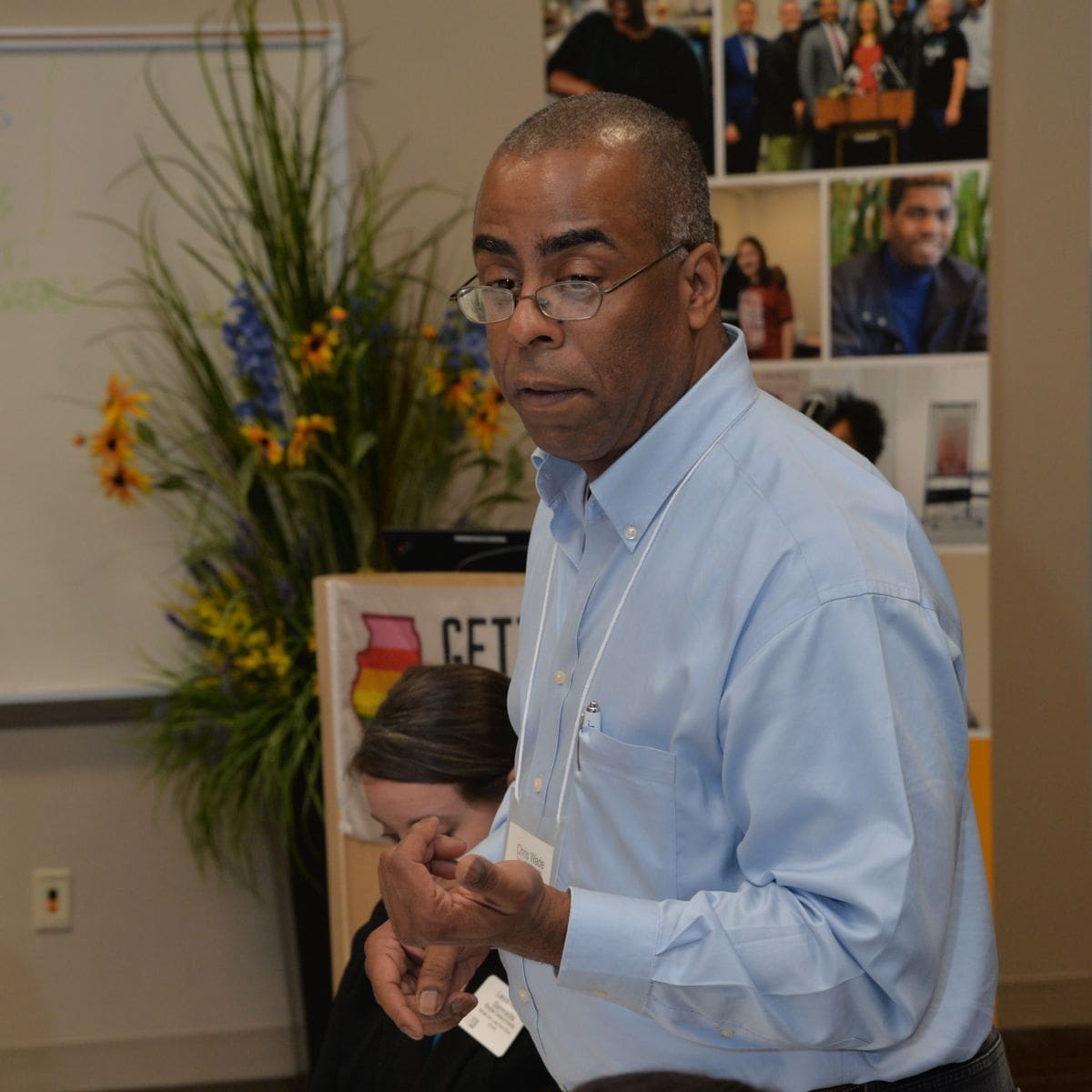 Chris Wade is more than just your average HIV advocate.
Chris Wade is more than just your average HIV advocate.
His longstanding work and organizing in downstate Illinois contribute to education and advocacy for the rights of people living with HIV. He attended the 2018 HIV is Not a Crime National Training Academy (HINAC 3) back in June in Indianapolis, Ind., which trained advocates from all over the nation to talk about the criminalization of people living with HIV. Chris shared his experience with us.
What was your experience attending HINAC 3?
From the beginning to the end, it was an amazing experience to be there. It’s always great to get around other people who are also living with HIV on a national level, but it’s even better when we’re connecting around a specific topic. The comradery really re-invigorates me.
Ending HIV criminalization has always been dear to my heart. It can happen to anybody at any point in time. So, the fact that we’re looking at modernization and repeal of these HIV laws, the intersections happening within intracommunity spaces experienced by people of color and those living with trans experiences. It’s just so important.
I also just love coming here for comradery, the opportunities to network with folks from out of state, establishing new relationships and tackling new stuff that hits in the moment.
Did you run into any challenges while attending HINAC 3?
I think the challenges really are, “How do we collectively have strategy that we can all get behind and be unified around?”
HIV criminalization was initially a federal issue. I think we, as advocates, are largely responsible for shaping the future of these laws — but it’s mostly on the federal government. Had they not created these laws initially, we would not be in the state of where we are today.
What was your day-to-day like for HINAC 3?
Each day was very different than the next, which I really enjoyed! Each morning, we gathered for breakfast and would attend the opening plenary of the day. Speakers from Colombia, Canada, Mexico, and all over came to talk about their HIV criminalization experiences ranging from immigration, sex work and the military. There were some newer, younger leaders that I spoke with that made me proud and offered me chances to encourage and affirm their work.
It was fun running into folks I’ve known for years, along with meeting new people and offering them some guidance, hope and nurturing to some of the newly diagnosed or new attendees. This is my second conference, and I really enjoyed myself.
The Black United Leadership Institute (BULI) group was always great to be around to connect, and uplift national work from Black-identified HIV advocates. They held a pre-conference before to train and encourage capacity-building on a national scale, which is a great addition from years past.
I appreciate spaces where I can see where people are at with their local advocacy efforts, and experience diverse representation.
How do you feel like you’ll take back the knowledge and experience gained at HINAC 3?
I want to go back to my local community and document their needs for HIV criminalization support. From that, I want to connect with partners and begin creating state-wide engagement strategies that may work to evolve these laws.
I appreciated the time HINAC 3 built out for advocates from each state to come together and strategize concrete steps to eliminate bad HIV laws. Illinois attendees, including myself, all sat around a table and talked about next steps and coalition-building incorporating information we heard from advocacy groups from places like California and North Carolina.
With more education and awareness targeting the community and state legislators, I think we can stop the unfair criminalization of people living with HIV. I think we’re starting to see Illinois advocates are investing in efforts to stop these discriminatory laws by bringing local community partners and individuals to the table.
What has your personal experience been with HIV criminalization laws?
Well, I’m currently the Director of Prevention Services at Central Illinois FRIENDS of PWA. We confirmed an allegation had been made in a local newspaper in my hometown of Peoria. We responded with a Letter to the Editor about the article to get it in the public eye how wrong it was.
The public health department and our agency jumped on it to really educate folks about modes of transmission, PrEP, and other relevant information. Some of the information that was put in the newspaper and other media outlets is stigmatizing and just diminishes all the work that we do.
Is there anything else you’d want people to know about this conference?
If you have the chance come to a HINAC, come to a HINAC. It’s a unique opportunity. You’ve got a mix of subject matter experts, advocates, policy makers, state representatives, and a lot of what I would call “HIV icons”.
Historically, you’ve got people who’ve been doing this work for a long time and been in this game a long time. And there’s a lot to learn from this model, but I keep finding that there’s still a lot of work we must do. We need more young and not-so-young folks to help shape this model to best support people living with HIV into positions of empowerment.
Want to get involved and learn more about Illinois’ efforts to end HIV criminalization? Contact Coleman Goode ([email protected]) for more information.
 Avery Matthew grew up in Sterling Heights, Michigan, and moved to Chicago 11 years ago. “I was starving for diversity, things to do, culture, museums,” they said.
Avery Matthew grew up in Sterling Heights, Michigan, and moved to Chicago 11 years ago. “I was starving for diversity, things to do, culture, museums,” they said.
“A lot of my growth and identification was defined in Chicago.” Avery works in Accounting and Finance recruiting for a management consulting firm. They also support passion projects like serving on the Chicago Women’s Health Center board of directors and as a co-chair on the Chicago Restroom Access Project (CRAP), an initiative of Pride Action Tank that’s creating new solutions to provide accessible bathrooms for all.
How has your move to Chicago shaped your life?
Here, you see a lot more eclectic folks who feel comfortable with who they are. Being exposed to an environment that allowed for such personal definition and evaluation gave me the permissions to feel what felt right. When I came out as gay in 2008/2009, I was in a relationship with a guy … so that was a little awkward!
Then, fast forward 7-8 years, and I went through another transition. Being seen as female didn’t give me a lot of comfort and I felt uncomfortable being held to socially assigned female expectations. I started doing some self-discovery and came out as non-binary two years ago. My pronouns are they/them. Not many people understand what identifying as non-binary means and each person who identifies as non-binary will have a different definition. As a result, you’re often responsible for explaining what it means and then serve as the model for it (even though there are a lot of variations).
I try to take an educational perspective with others — assuming people are asking kind, respectful questions. I like expanding the mindset there. It can be hard existing as non-binary because people want to see you as either a man or woman. It leads a lot into the CRAP committee.
How did you first hear about CRAP?
I was at a summer festival in Boystown in 2016 and got to talking to someone who worked at the AIDS Foundation of Chicago (the parent organization of Pride Action Tank). I got in touch with Pride Action Tank’s executive director, Kim Hunt, and she started talking about CRAP and I had a lot of feelings about it! It would really help me and a ton of my friends, as well as my community to get things changed.
CRAP is focused on growing the number of all-gender bathrooms in Chicago. Why does equal bathroom access matter to you?
I’m on T (testosterone supplements to change my body) now, but even before starting T I always had short hair and wore guys’ clothes. Going into restrooms or spaces that are gendered as male or female has always been anxiety producing. I’ve been told, “this is the women’s bathroom,” or have had people stop in their tracks and look at me with a scared look. I’ve even been kicked out of a bathroom. I can’t avoid the bathroom so I go in with my head down, avoid eye contact and washing my hands, and get out as soon as I can. Bathrooms are perceived to be very personal, vulnerable spaces so it scars you when you have encounters like I have.
You were kicked out of a restroom?!
It only really happened once, but that one time scars every other time. It actually happened when I was working for a LGBTQ group that threw parties in traditional straight spaces where we’d convert it to a gay bar for one night. When possible, we tried to turn bathrooms into all-gender bathrooms. We weren’t always able to, so we instructed staff at the spaces to not stop anyone from going into bathrooms. But at one space, the bathroom attendant in the women’s room grabbed my arm. It was good and bad that it happened because it provided an opportunity to educate the staff.
Bathrooms are one of the hardest part of living how I do. There are no public restrooms for me. Both of the current options feel wrong. I feel safer in the women’s than I would in the men’s, so that’s the one I want to go to, but as I continue to change and be on T, I may lose that privilege.
Tell me more about CRAP! What have they accomplished?
In the early days of CRAP, the group started out by partnering with Chairman and Commissioner on the Commission of Human Relations Mona Noriega, who was already working to overturn a law that said you could be asked to show a photo ID in a bathroom to prove you were in the right one. Now you are not allowed to ask someone for their ID in a restroom, and they’ve done a lot of education and trainings with police and libraries.
Wow — that’s huge. But then they shifted their focus to all-gender restrooms, right?
Yes — a lot of people don’t realize that a restaurant that has at least two single-stall restrooms must label one for men and one for women. But it doesn’t make sense why this is the case since there is privacy in each. Turns out that the building code specifies that businesses have to have individual bathrooms for men and women if there are multiple single-stall restrooms. In the past they could be fined for not having separate bathrooms. We surveyed a lot of businesses to learn whether they would change their signage if we got this change made.
So CRAP amplified the work that Commissioner Noriega has done to get the commissioner who oversees this code to agree not to prosecute. This is a big thing to the community! Now we’re working on eliminating the gendered verbiage in the code, but we’re happy with what we’ve done for now. We want to partner with more architects to think about how to work around the system. That was our most recent thing. But people have to spread the word, too! That’s next on our list.
What does CRAP do to inform businesses about these rights?
We have created a toolkit that explains to business owners the concept and benefits of all-gender bathrooms. We’ve had businesses reach out to us to help them assess and consult with them about changing their restrooms or add signage to show their support. The toolkit helps them with their bathroom planning.
We’re also creating a video project where we interview people who are transgender or those that present masculine of center to learn about their experience with bathrooms. This video will be used for educational and awareness purposes. We’ll be targeting different markets, like schools and restaurants, to show the video in hopes of influencing them to adopt all-gender restrooms or direct them to additional resources to continued research.
The day-to-day operations of the AIDS Foundation of Chicago focus on improving access to services for people living with and vulnerable to HIV and other chronic illnesses; this vision emerges from AFC’s 27-person Board of Directors. These community leaders bring a variety of skills and interests to cast the vision for the organization and lead it in achieving its mission. In 2018, the Board welcomed seven new members to its fold; we invite you to meet them below!
If you have any questions for the AFC Board or want to learn about how you can join, please reach out to AFC President & CEO John Peller.
 |
Geoffrey E. Brown, CAE, is the CEO of the National Association of Personal Financial Advisors (NAPFA). In this role, he is responsible for the association’s strategic direction, external relations, and ensuring its operational success. He is also a member of the Association Forum of Chicagoland, where he serves on the Board of Directors as Secretary-Treasurer. Brown also serves as Treasurer on the Board of Directors of the Association of Fraternal Leadership and Values. |
 |
Lance Glass is the Manager of Cost Accounting for Luster Products. Previously, he served as Vice President of Finance for There is a Need, a nonprofit he cofounded to support the African American community to combat HIV/AIDS. There is a Need developed programs to help individuals with all their needs, including everything from medical to shelter. He also works as the chairperson of the men’s chorus at Trinity United Church of Christ in Chicago, where he manages the daily operations of this $60,000 ministry area. |
 |
Paris Mullen is a Community Liaison for Merck. In this role he provides capacity building support for case managers and other allied health professionals who serve communities living with HIV and/or Hepatitis C. He is also the CEO and founder of Hope for US (parismullen.org). This organization is dedicated to developing hope and self-worth for individuals dealing with psychological, spiritual and emotional challenges of living with trauma. |
 |
Mary Pounder serves as the Program Director at the Comer Family Foundation. Here, she directs the grant making and relationship management for the organization and collaborates with over 180 non-profits to make a lasting impact on the lives of individuals and communities throughout Chicago and nationwide. She has a distinct dedication to harm reduction among people who inject drugs and expresses her commitment to equity and justice as a Committee Member of Human Rights Watch. |
 |
Tom Sondergeld is currently the Vice President of Global HRIS, Benefits & Mobility for Walgreens Boots Alliance (WBA). Tom has directed employee benefits for over 20 years. He has spoken at many local and national events on topics ranging from benefit plan design, wellness integration, and on-site health centers. He is currently the acting Chair for Midwest Business Group on Health. |
 |
Tony Tintinalli has had a very successful career in banking since 1998. He joined BMO Harris Bank from Canadian P&C in January 2017 when he stepped into the newly created role of Head, U.S. Premier Sales to deepen relationships with customers with investable assets between $250,000 and $1 million. Previously, Tony served as Regional Vice President for Toronto Downtown, which is the largest retail banking market in Canada. |
 |
Dr. Karriem S. Watson, DHSc, MS, MPH, is a Senior Research Scientist with the University of Illinois Cancer Center and the Director of Community Engaged Research for the UI Cancer Center at UIC and the Mile Square Health Center. Dr. Watson’s work has resulted in the creation of community-based cancer screening, prevention and navigation programs. His work afforded him recognition by the Metropolitan Chicago Breast Cancer Task Force as a “Community Champion.” |
 Over the course of the last two weeks, Governor Bruce Rauner has deemed it necessary to veto three pieces of health care access and treatment legislation that would have had a positive and meaningful impact on the lives of people living with chronic illnesses, including HIV. The disappointment we feel in the Governor’s actions is tempered by the knowledge that all of these bills will have the opportunity to become law when the AIDS Foundation of Chicago (AFC) and our partner agencies join with our legislative sponsors to override these vetoes in the November veto session of the Illinois General Assembly. With three strokes of the pen, the governor did away with drug access protections for people living with chronic illnesses, allowed junk insurance to thrive in Illinois, and revoked a role for the General Assembly in health care waivers that impede or diminish health care benefits.
Over the course of the last two weeks, Governor Bruce Rauner has deemed it necessary to veto three pieces of health care access and treatment legislation that would have had a positive and meaningful impact on the lives of people living with chronic illnesses, including HIV. The disappointment we feel in the Governor’s actions is tempered by the knowledge that all of these bills will have the opportunity to become law when the AIDS Foundation of Chicago (AFC) and our partner agencies join with our legislative sponsors to override these vetoes in the November veto session of the Illinois General Assembly. With three strokes of the pen, the governor did away with drug access protections for people living with chronic illnesses, allowed junk insurance to thrive in Illinois, and revoked a role for the General Assembly in health care waivers that impede or diminish health care benefits.
HB 4096, sponsored by Representative Greg Harris (D-Chicago) and Senator Heather Steans (D-Chicago) passed both chambers of the General Assembly with bi-partisan support. The bill sought to prevent the state from restricting the drugs available to Medicaid members starting January 1, 2019, by imposing a more restrictive single preferred drug list on all Medicaid Managed Care Organizations. We must override this veto to ensure that people living with chronic illnesses have access to as many life-saving treatments as possible.
HB 2624, sponsored by Representative Laura Fine (D-Glenwood) and Senator Heather Steans (D-Chicago), sought to regulate short term limited “junk insurance” health plans in Illinois, make it plain to consumers that these plans did not meet the requirement of the Affordable Care Act (ACA) and limit their availability to 6 months. These plans provide little to no benefits to the people who purchase them, and the Trump Administration just allowed people to buy them for up to three years. Gov. Rauner’s veto is a blatant attempt to allow harmful Trump administration policies into Illinois, which will undermine ACA marketplace plans with long term and lasting consequences.
HB 4165, sponsored again by both Representative Greg Harris (D-Chicago) and Senator Heather Steans (D-Chicago), required the Governor to gain legislative approval before submitting any waiver to the federal government that would allow the state to diminish or impede an existing health care benefit. By vetoing this bill, the governor seeks to retain full authority of the executive to seek any waiver to the federal government, even if it strips Illinoisans of their existing health care benefits.
“Governor Rauner’s actions are disappointing and dismaying,” said John Peller, CEO of the AIDS Foundation of Chicago. “But we are not disheartened. We are confident that the General Assembly will come together in November and vote to protect the people of Illinois from disastrous policies being handed down from both our state and federal executives. It’s imperative that the General Assembly override these vetoes and protect the most vulnerable among us.”
 AFC staff and Board were saddened to hear of the passing of our long-time partner and dear friend Dan Bigg. Dan, the founder and executive director of the Chicago Recovery Alliance (CRA), was a brilliant, passionate, persistent and formidable advocate who will be never be forgotten by the many thousands of people whose lives he touched. We stand in solidarity with his family and CRA staff and clients. And we dedicate ourselves to continuing the fight against HIV with the grit, determination and humanity that Dan fostered.
AFC staff and Board were saddened to hear of the passing of our long-time partner and dear friend Dan Bigg. Dan, the founder and executive director of the Chicago Recovery Alliance (CRA), was a brilliant, passionate, persistent and formidable advocate who will be never be forgotten by the many thousands of people whose lives he touched. We stand in solidarity with his family and CRA staff and clients. And we dedicate ourselves to continuing the fight against HIV with the grit, determination and humanity that Dan fostered.
CRA was one of the first organizations in Chicago to offer syringe exchange programs, which dramatically reduced transmission of HIV and hepatitis C among people who inject drugs. Dan pioneered distribution of naloxone, a drug overdose reversal drug. His bold and visionary programs, always promoting compassion, empathy and “any positive change,” proved that lay people could be trained to administer naloxone to save the lives of their friends and family members. Naloxone distribution programs have since spread nationwide as a critical response to the opioid crisis. Most recently, Dan was focused on creating safer injection spaces based on successful global efforts.
Dan made many firsts possible, but ultimately, he will be remembered for building an organization that fostered respect and dignity for people who use drugs. In partnership with AFC, he championed two state legislative issues that dramatically impacted the trajectory of the HIV epidemic in Illinois. In the late 1990s and early 2000s, AFC and CRA led a successful fight in Springfield to allow the purchase of sterile syringes over the counter at pharmacies without a prescription across Illinois. AFC and CRA in 2009 worked to pass legislation that legalized the naloxone distribution programs that Dan had pioneered.
Check CRA’s Facebook page for more information. https://www.facebook.com/chicagorecoveryalliance/
To donate to CRA in Dan’s memory, click here: http://www.anypositivechange.org/give.html
 Today, the AIDS Foundation of Chicago (AFC) is deeply disappointed that Gov. Bruce Rauner is playing political games with the lives of millions of Illinois residents who rely on the Medicaid program for access to their lifesaving medications, including people living with HIV.
Today, the AIDS Foundation of Chicago (AFC) is deeply disappointed that Gov. Bruce Rauner is playing political games with the lives of millions of Illinois residents who rely on the Medicaid program for access to their lifesaving medications, including people living with HIV.
Sign this petition now to urge legislators to override the governor’s veto
Gov. Rauner issued a veto Monday, Aug. 20 of HB 4096, which seeks to prevent rationing of health care by the state. The bill would block an effort by the state to require Medicaid managed-care organizations (MCOs) to use a single Preferred Drug List (PDL).
PDLs establish which drugs are available to patients without prior authorization or other utilization controls. Today, Medicaid MCOs may institute their own unique PDLs, which are nearly always more generous than the state’s fee-for-service PDL. Illinois in 2017 proposed requiring all MCOs to follow the state’s stingier fee-for-service drug list, which would institute barriers to care for millions of Medicaid recipients by limiting the number of drugs they could access.
The bill was sponsored by Rep. Greg Harris (D-Chicago) in the House, where it passed 70-31, and by Sen. Heather Steans (D-Chicago) in the Senate, where it passed 47-9 with bipartisan roll calls. AFC pledges to work closely with legislators to override the Governor’s veto during the fall veto session, scheduled for November 2018. Just one additional vote is needed in the House to overcome the veto: the Senate previously passed the bill with a veto-proof majority.
Under a single PDL, Illinoisans living with chronic illnesses like cancer, HIV, mental health challenges, opioid dependency, diabetes, hypertension and many other diseases would be forced to put important health care decisions in the hands of the state instead of between patients and their health care providers. A single PDL would also impose more burdensome administrative requirements for prior authorizations on providers and increase nonadherence to medication for patients, because it creates unnecessary obstacles to care. A single PDL is not practical, and it dangerously obstructs a patient’s ability to adhere to the care recommended by their health care provider.
The state’s proposal is particularly harmful for people living with HIV, as the state allows direct access to just two single-tablet HIV medications, while all the MCOs have a least five of the six on formulary. One-pill, once-a-day single-tablet medications promote adherence to HIV treatment, which is vital for maintaining the health of people with HIV and preventing transmission of HIV. Click here to explore AFC’s MCO HIV drug guide.
Additionally, HB 4096 would make transparent the process in which recommendations are made to the Department of Healthcare and Family Services (HFS) on which drugs are included on the state’s PDL.
Illinois is currently the only state in the nation with a closed, secretive Drug & Therapeutics (D&T) Committee, which removes a critical avenue for patients and providers to advocate for access to medications. The bill would subject the D&T Committee to the Freedom of Information Act and the Open Meetings Act.
“Gov. Rauner is using his executive powers to restrict access to critical medications for millions of Illinois residents. The governor’s veto will result in fewer people living with HIV on Medicaid achieving viral suppression and will undoubtedly result in more people becoming HIV-positive, moving us further away from our goal of reaching zero new transmissions of HIV by 2030,” said John Peller, CEO/President of AFC. “We will not sit idly by and allow artificial administrative barriers to lifesaving medications to be erected. We will work diligently this fall to secure the votes needed to override the Governor’s veto during veto session,” says Peller.
Join us in this effort by signing our petition telling legislators to override the governor’s veto of HB 4096.
Click here to sign our petition!
 The AIDS Foundation of Chicago (AFC) coordinates 135 case managers throughout the Chicago metropolitan area to support clients who are living with HIV and related chronic diseases. Case managers are there to connect with clients directly and help them achieve goals such as obtaining stable housing or getting connected to a medical provider that may help them reach an undetectable viral load. Because they do so much for our communities, AFC’s Communications Coordinator, Raven Feagins, sat down with a case manager from Chicago House and Social Service Agency – an organization dedicated to supporting the well-being of people living with HIV, the LGBTQ community and other underrepresented communities – to learn more about what goes into helping the hundreds of clients AFC’s partner agencies see every year.
The AIDS Foundation of Chicago (AFC) coordinates 135 case managers throughout the Chicago metropolitan area to support clients who are living with HIV and related chronic diseases. Case managers are there to connect with clients directly and help them achieve goals such as obtaining stable housing or getting connected to a medical provider that may help them reach an undetectable viral load. Because they do so much for our communities, AFC’s Communications Coordinator, Raven Feagins, sat down with a case manager from Chicago House and Social Service Agency – an organization dedicated to supporting the well-being of people living with HIV, the LGBTQ community and other underrepresented communities – to learn more about what goes into helping the hundreds of clients AFC’s partner agencies see every year.
Lakethia Conner is a passionate, family-oriented mother of one who resides in Chicago’s Roger Park neighborhood. She was born and raised in Chicago’s Cabrini-Green homes, where she grew to understand the value of a close-knit community as well as the importance of having access to the necessary resources to thrive and live a healthy life. She attributes her upbringing, along with lessons learned about acceptance and equality, from her grandmother, to her desire to enter the world of social services where she has been working as a medical case manager for the past 2 years.
Q: How would you describe case management to people who don’t already know?
A: There’s different types of case management, but overall (under the umbrella) a case manager is someone who basically advocates, provides support and connects their clients to services.
A medical case manager is someone that is involved in their client’s all-around life but focuses on medical to make sure that they’re adherent to doctor’s appointments, medication and just in general getting healthier.
Q: How many clients do you work with now?
A: Right now, I have 33 individuals. I am also supervising Chicago House’s new program of non-medical case management, so that is a case load of 40 I believe.
Q: What kind of things do your clients come to you for?
A: It’s a very wide range! My case load has ranges from some self-sufficient people to people experiencing homelessness. I get requests for rental assistance – whether a person is going from homelessness to housing, whether it’s subsidized housing or some type of housing program … or maybe they lost their job and need assistance to help pay rent and utilities until they find another position. Health insurance is also a big, big thing – there’s a lot of questions regarding insurance. Also, food services – whether it’s hot meals or food pantries.
Q: Is housing one of the larger issues that you have to tackle?
A: It is. Working previously at Housing Opportunities for Women with the housing-first model and being in my position as the patient navigator … I’ve witnessed that once a person is housed, everything sort of falls into place. But I know that Chicago has limited affordable housing, which sucks, so yeah, housing is one of the most difficult pieces.
Q: What is a typical day like for you here?
A: It depends of which day of the week. I’m co-located at UIC, which has two medical providers who do morning clinics 2 – 3 times a week. Clinics are days that the doctors are in the clinic and seeing patients/clients. I’m available during clinic hours so clients could do everything on the same day.
Mondays there’s the afternoon clinics, so Monday mornings I’ll come in and there’s always work to do. I check my voicemails because clients … they’ll call at midnight and some of them will just be like, “I just want to address this first thing Monday morning.” So, my Mondays are just catching up on all of those messages. If there’s a fire, giving that attention, but there’s always case notes to do, there’s always phone calls to return or someone to track down. Then lunch (hopefully) happens, then afternoon clinics.
Tuesday there is morning clinic, so I know if any of my clients or anyone that needs assistance with ADAP or anything, they will be in that day. I try to prepare the paperwork because if there’s five clients waiting on me, it’s easier to just have the paperwork done and that just makes the day and time just move. Then, I’m able to see everyone without them waiting a long time or getting irritated. I try to be prepared.
I try to do all of my appointments here at the clinic or one of the Chicago House locations, but when I did have a few homeless clients with no income, I would go meet them out in the community.
It’s basically just always being here and being available. There’s always paperwork and always things to enter and issues that come up.
Q: What motivates you to continue doing this work?
A: It’s easy for me. I had a career change from certified medical assistant phlebotomist and an EMT and I managed an outpatient county clinic for four years or so.
My grandma always called me the helper, so this work comes so naturally for me. And to get paid for it, it’s great. I think burnout is always on the edge, but self-care helps with that.
Q: What do you do for self-care?
A: It depends how the wind blows! I have a good sense of humor – and I try to keep that. Also, baths are really, really relaxing — and sunshine. If there’s no sunshine, I can have off days. Just give me some sunshine, a glass of wine and a bath and I’m good.
Self-care is the most important and I think my clients … they understand and so does my family. If I feel that I don’t have the best resources or attention at that time, I will call you back when I know I can be that person. Also shutting my phone off. I will do it in a heartbeat now. It took me a while to do, but … yeah. Boundaries.
Q: What’s the most challenging part about your job?
A: The most challenging for me, it’s when I give a person every tool they need and they’re just not utilizing them. That’s challenging for me. It makes me step back and re-assess and have real and honest conversations with the person to figure out what the issues are. I’m a problem-solver so just being honest with the person is almost getting to the root of the problem. Once they know you’re sincere and know that you really care, they’ll usually open up.
Q: What’s one of the most rewarding parts about your job?
A: The rewarding thing is when someone utilizes all of the tools and just becomes self-sufficient! Just to see growth in an individual is like, “Yay!”
To learn more about case management and other services coordinated by AFC, please click here to visit our case management page.
This interview has been condensed and edited for brevity and clarity.
HIV Prevention Justice Alliance (HIV-PJA) started 11 years ago with the “radical notice” that all people should be treated equitably, and all people deserve social justice. This 13,000-person network was born intentions to unite advocates across the country to address the intersections of HIV/AIDS and economic, racial and social justice.
We are saddened to announce that HIV-PJA will end its service as the lead entity in this fight as of today (Monday, Aug. 13, 2018).
Over the years, this network grew into a community of people living with HIV, as well as activists, advocates, researchers, health care providers and policy-makers working at the intersection of HIV/AIDS and social justice in the U.S.
Now, this movement lives with in all of us — and our actions of resistance. The fight is not over; today, we are experiencing an intense time of blatant assaults on our communities, especially people of color, people with inequitable access to health care, people and families with undocumented immigration statuses, and the LGBTQ+ community. However, we at the HIV-PJA family believe this next part of our journey to end the epidemic lives within the collective action of the HIV community and no longer in the confines of HIV-PJA.
HIV-PJA may be sunsetting today, but the many movements locally and nationally that make this fight possible with continue to exist long after today. We encourage you to connect with the lead organizations behind HIV-PJA to continue to learn how to serve the national movement to improve the lives of people living with and affected by HIV:
– AIDS Foundation of Chicago
– AIDS United
– Desiree Alliance
– Drug Policy Alliance
– Harm Reduction Coalition
– Positive Women’s Network
– SisterLove, Inc.
– Treatment Action Group
This is what democracy looks like!
With gratitude and hope,
HIV Prevention Justice Alliance
For any questions please feel free to contact Kirstin Brockenborough, Policy Communications Specialist ([email protected]) and Ramon Gardenhire, Vice President of Policy and Advocacy ([email protected]).

Brandon
My name is Brandon Strawn, and I pride myself on being an educator, a musician and a delight. In 2005, I came out as gay, and in 2009, I had my first HIV test. At this point in my life, I was a fairly chaste first-year teacher who spent his days teaching and his nights preparing for more teaching. So when the test came back positive, I was shocked and devastated. How could this have happened? I would now never find a husband, could now never have biological kids and would probably die decades early. I spent the following days severely depressed, reaching out to close friends and family and desperately pleading with reality that this was a horrible dream.
Ten days later, I returned to get the results of my Western blot test and received another surprise: they were negative. I had received a false positive on a 99.7% accurate test. I had dreamed of nothing more than waking up from that nightmare, and then just like that, I had done so.
By early 2017, I decided to be even more responsible than I already considered myself to be. While I still got tested regularly and thought I didn’t take any serious risks, I had heard about PrEP and decided to get a prescription. I also happened to be quite sick with the winter flu, and I thought I could maybe get some medication for that. I dragged my flu-ridden body in to get tested again to get a prescription for PrEP and quickly found out that apparently I was too late. The most recent guy I had been with, and shown my negative status to, didn’t actually know his status as well as he had thought, and the flu I thought I had was actually the virus seroconverting into my body. I was now HIV-positive. No pleading or dreaming would get me out of this one.
Within a few hours of being diagnosed, the Howard Brown Health Center provided me with a veritable troupe of medical experts, several vaccinations, and over $5,000 of medication, all for free. Next when I started telling the several people close to me, everyone–family and friends, liberal and conservative–responded with understanding and support. It occurred to me that I had gone in to take a pill every day to prevent spreading HIV, and now here I was, doing just that. This pill has lowered my viral load from an initial intake of 284,000 counts per mL of blood to under 20. Not 20,000. 20. I am now undetectable, untransmittable and understanding of how the stigma had impacted me — and how I can use my story to combat it.
Daniel
My name is Daniel Eggert, and I am a small-town boy from Indiana. When I moved to Chicago in 2013, one of my friends found out I enjoyed running and invited me to run the Bank of America Chicago Marathon with him, to raise money for the AIDS Foundation of Chicago through TEAM TO END AIDS. After signing up, I made some new friends through the charity and I also learned so much about HIV, AIDS and this new(ish) pill called PrEP, which HIV-negative people can take daily to prevent contracting HIV. I decided to go see my doctor and ask about getting a prescription. I have now been on the medication for 5 years, but at one point during the 5 years, I was in Indiana and had to go see a doctor while I was there. During my visit, I was asked what medications I was on and I told her about the PrEP. The doctor first got confused, then judgemental, and didn’t like that I was taking the medication. She shamed me for taking a medication as a precaution and taking care of myself. I have not been back to see that doctor since I didn’t feel comfortable talking to them about anything. I couldn’t believe there was even stigma against safe sex in the medical field!
I finished my last year of college and moved back to Chicago once I found a job. During that time, I had started seeing someone who lived in the city. I spent a lot of my time with this guy; we decided together that things were going well and that we didn’t need to use protection when we slept together. In my mind, that meant that we were monogamous. I found out later that I was wrong. He had been sleeping with several other men as well. I ended that and decided to focus on the new city and life I was going to make for myself. The next several years were crazy, fun and stressful. But in 2017, one night changed everything.
Brandon
By April 2017, I was on my way, but I wasn’t undetectable yet and had serious reservations about dating. I was determined to be a Hester Prynne, but I let friends drag me out to Boystown anyway. We were standing around drinking and chatting at Progress, when eventually one of their friends arrived. He stood on the other side of the circle of people. He was tall and red-headed and couldn’t talk without bashfully smiling and chuckling. My first thought was “well, he’s far too handsome to be single.”
Daniel
That night, my friends took me to Progress in Boystown, and I ran into some other friends who introduced me to their group. While I was standing there swaying to the music, I noticed a handsome guy that seemed to be with my friends. I leaned over to my friend and told her that I thought he was handsome. She said “Really? I think he is single. Let me work my magic!” I said okay and joined my other friends in the back bar for a little while.
Brandon
At one point, he walked away, and one of my friends came up to me and flirtatiously asked “do you think Daniel is handsome?” I gushed and said yes. “He thinks you are too! You’re single, right?” I didn’t want to go into details about my status and how someone like me didn’t deserve love… So I just said yes. She replied: “Let me work my magic!”
Daniel
My friends and I went back up to the front bar, where my friend gave me a wink and brought me back into the circle. I found myself standing next the handsome guy, summoned some courage, leaned over and said “I think you are very handsome.” He blushed and returned the compliment.
Brandon
The rest of the night, our friends blurred out into the background as Daniel and I talked for hours. Then went on a date. Then more dates. A few weeks went by, and I could tell we were ready to take our budding relationship to the next level, but I wasn’t undetectable and hadn’t told him yet and didn’t feel comfortable being intimate with him. So one night, I worked up my nerve to continue my responsibility and tell him my status. I chose my words carefully and didn’t want to martyr myself, but I pleaded internally that this news wouldn’t be a dealbreaker.
Daniel
That night, Brandon seemed to be quiet and a bit nervous. I wasn’t sure what was going on. He said that he had something to share. He told me that he was HIV-positive and then cautiously waited for a response from me. At this point, my education on the subject allowed me to patiently and calmly reply “that’s okay. I’m on PrEP.” I explained that I knew more than most on the subject, and immediately saw him relax.
* * * * *
Now we have been together for more than a year as a magnetic couple, (one positive and one negative). We are honored to share our story with the world while both running the Bank of America Chicago Marathon, raising money to end the HIV epidemic and to end the stigma that surrounds it. Our hope is that sharing our story will encourage others to share their stories as well. After all, it is only by knowing more of us that the world will overcome the stigma and understand the reality of preventing and responsibly living with this treatable virus. We will all make it to this finish line together.
To support Brandon and Daniel in their race to the finish line, please visit http://bit.ly/brandanmarathon