The AIDS Foundation of Chicago (AFC) is proud to announce the 12 organizations selected to receive non-medical case management funding to serve people living with HIV throughout the Chicago metropolitan area. Organizations will be receiving funding through the Ryan White HIV/AIDS program, which distributes $2.3 billion nationwide to fund services specifically for people living with HIV. This funding will allow case managers to further assist clients who are self-sufficient and do not need intensive services, but need occasional support such as insurance enrollment, medication assistance application help, short-term medical or housing payment assistance and much more.
“This funding expands the reach to vulnerable clients who have traditionally not been the priority of case management funds, but have a great need,” said Bashirat Osunmakinde, AFC’s senior director of Care.
This year, AFC received 19 applications from organizations, and the selection process was no small feat. Applications were reviewed by multiple entities, including a first round of reviews by members of the Chicago Area HIV Integrated Services Council (CAHISC), individuals unaffiliated with AFC (but who have HIV/AIDS work experience) and non-Care team staff at AFC. After the applications were ranked by each of these groups, AFC’s Care, senior leadership and program development teams reviewed applications and took into account the rankings of the review panelists before making their final decisions.
“Organizations selected for this year’s awards were ones that already had an established client base, have a strong fiscal and administrative support staff and clearly documented the need for funding,” said Osunmakinde.
It was also noted how important it was to award organizations that represent the breadth of communities served by AFC partner organizations throughout the entire Chicago metropolitan area. In order to make the biggest impact, it was crucial to application reviewers that work would be funded to organizations not only in downtown Chicago but also in places where services may be scarce.
“Over the course of the HIV epidemic, the face of people living with HIV and the communities most impacted by it has shifted,” said Román Buenrostro, AFC’s director of special projects and planning. “We feel very proud that the organizations selected to provide this new level of care reflect the diversity of the communities currently impacted by HIV in Chicago.”
Ultimately, AFC is dedicated to continue growing and building relationships with partner organizations throughout the Chicagoland area and beyond. These RFP awards allow for those partnerships to stay intact and for organizations to continue providing services for people living with HIV.
 By Raven Feagins
By Raven Feagins
When the weather is nice, Donald King bikes over to Lake Michigan to go fishing. It brings him back to memories of his childhood in New Orleans and spending time with his mother before she passed away. His charming smile and laid-back personality could fool anyone into thinking that he has lived an easygoing life, but he’s had an arduous journey that has led him to where he is today.
Donald moved to Chicago’s North Side in the late 1950s when his mom decided to relocate the family in hopes of finding better schools and better job opportunities. While the change was tough at first, Donald adjusted and made Chicago his home. He went on to graduate from high school in 1975 and soon after got married and had his first son. Over the next few years of his young adult life, Donald worked full-time but was later laid off due to a company shutdown. He then found work at a video service and technology company in the 80s, but it wasn’t long before his hours became more and more scarce. Nonetheless, Donald still managed to support his growing family through the years.
“I was working in the 90s off and on, but my wife, she worked for a long time,” says Donald. “We had two kids then, so I took care of the kids, I took care of the house until she came in from work.”
This lasted until Donald had a run in with the law and he went to county jail for 6 months. Upon his return, he found that his wife wanted him to move out of the house and to get a divorce. Donald moved in with his younger brother and then with his older brother, still in search of consistent, full-time work. However, with the recent charge on his record, Donald’s job search became even harder.
“I didn’t have nothing but my Link Card … I couldn’t get a job at the time because I was on three years’ probation. I tried to get a job, but they wouldn’t hire me,” says Donald. “Mostly what I did was stay at home and go fishing.”
In 2012, Donald moved out of his brother’s house and retreated to a men’s shelter in Chicago’s Uptown neighborhood. He lived there for almost 4 years until he was told that he needed to find work in order to stay, but, again, Donald was unable to secure a job. With nowhere left to go, he decided to make the move to the Lawrence Avenue viaduct where a few of his other friends who were also experiencing homelessness started setting up tents in what was called Tent City.
Several of these encampments emerged under Uptown viaducts and served as a makeshift shelter solution for dozens of Chicagoans. Tents of various sizes, shapes and colors lined the sidewalks and created a sense of community among residents.
“When I lived in Tent City, we all looked out for each other to make things right,” says Donald.
He tried to make the best of his situation, but the effects of living on a busy Chicago street for a year took a toll on Donald’s health. He was constantly concerned about protecting his belongings from being stolen, keeping out the rats that frequented the area and, overall, staying safe because he had no real sense of protection or privacy. Due to the constant stream of stress, Donald’s anxiety and high blood pressure were in full gear that year, but he never addressed his health concerns because he was so focused on surviving to the next day.
“It’s helped with my nerves, my blood pressure … I’m more relaxed, more safe,” says Donald in reference to his new home. “I get a good night’s sleep. I don’t have no problems like I used to have … I don’t worry no more.”
“You’re living out in a tent, you know. You never know what’s going to happen. You have to look out,” says Donald. “Imagine you being homeless; It’s rough! If you don’t know nobody and you’re broke … It’s rough!”
Moving into an apartment was always on Donald’s mind, and he spoke to several representatives from Uptown-based social service organizations, who frequently visited Tent City residents, about his goal. However, whenever the possibility of connecting to housing came up, most organizations only had available units on the South and West sides of the city. This was a huge problem for many Tent City residents who, like Donald, call the North Side of Chicago home. He wanted to stay close to everything he knew, but more importantly he wanted to stay connected to his family.
“That’s where my family was … I don’t really know nobody out West. I don’t really know nobody out South. So, why should I have to move out there? Probably better apartments, but it ain’t worth it,” says Donald. “I went to school around here. Grammar school, high school – I know a lot of people out here … so I decided to be patient.”
When August 2016 rolled around Donald found out that he was approved to be part of the Better Health through Housing (BHH) program. He was connected to his case manager through H.O.W., who worked with Donald to stay on the North Side of the city. He immediately moved into temporary housing in the Edgewater neighborhood and lived there for close to 5 months. During that time, Donald worked with his case manager to address his health concerns and waited patiently as they searched for his new home.
January 2017, Donald moved into his 1-bedroom apartment and has since seen noticeable improvements to his health.
“It’s helped with my nerves, my blood pressure … I’m more relaxed, more safe,” says Donald in reference to his new home. “I get a good night’s sleep. I don’t have no problems like I used to have … I don’t worry no more.”
Since his move, Donald is able to stay connected to his children, grandchildren and continue to indulge in his love for fishing. In the long-term, he hopes to move back to New Orleans and reconnect with his roots, but, for now, he is focused on finding a full-time job, managing his health and enjoying the comforts of having a place to call home again.
Update: IDPH released budget information and responded to AFC’s FOIA request. Click here to read our findings.
How has the Illinois Department of Public Health spent the $25 million in state funds budgeted for HIV services in FY18? The AIDS Foundation of Chicago (AFC) doesn’t know, and we’re disappointed in this lack of transparency regarding taxpayer dollars and needed services for those living with and vulnerable to HIV.
Despite numerous requests, IDPH has not provided a public accounting of the spending of public state tax dollars granted under the authority of the budget for the current fiscal year to the HIV Lump Sum, passed by the General Assembly in July 2017. Due to the lack of the state’s transparency unfortunately AFC has been forced to file a Freedom of Information Act (FOIA) Request to obtain this information.
The HIV Lump Sum supports vital HIV testing, prevention and outreach services, as well as linkage to health care and other services that prevent HIV transmission and help communities most affected by HIV thrive. Community-based organizations, health care providers and health departments provide these services across the state’s 102 counties. Approximately 45,500 people are living with HIV in Illinois.
Illinois has made significant progress in the treatment and prevention of HIV in the state, with the advent of new prevention technologies such as Pre-Exposure Prophylaxis (PrEP), treatment as prevention and the development of Illinois’ first “Getting to Zero” statewide plan aimed at eliminating new HIV diagnoses in the state over the next decade. However, particular communities continue to be most impacted by HIV.
- Nearly 70% of new HIV infections are in the Black and Latinx communities
- According the DPH, nearly 40% of new HIV cases are among young people 20 – 29
- Most alarmingly, HIV rates are highest among young gay and bisexual Black men, and a recent report highlights that a young Black gay man becoming sexuality active today at the age of 18 has a 60% chance of being HIV-positive by the age of 40. In addition, a recent study suggests that 66.7% of Blacks between the ages of 18 and 65 years old have never been tested for HIV.
Given these numbers, the state should use ever tool available to fight the HIV epidemic. Since the inception of the HIV Lump Sum, IDPH has made a public accounting of its spending every year, even during the two-year budget impasse from 2015-2017. That is now refuses to do so is truly troubling, and goes against the spirit of cooperation that was established in creating of the HIV Lump Sum.
AFC will share with the community the information we receive from our FOIA request. AFC calls on the Illinois Department of Public Health to release a full accounting of its spending under this portion of the Department’s budget, so that the Department and the community may work together to best address the HIV epidemic in Illinois by spending every state dollar available for that purpose where it is most needed.
Helping people leaving Illinois’ jails and prisons thrive is at the core of the Safe & Sound Return Partnership (SSRP), a three-year program that started in October that will connect 215 returning citizens Led by the AIDS Foundation of Chicago (AFC) and funded by a $900,000 federal grant from the Health Resources and Services Administration (HRSA), SSRP will also partner with and train citywide housing and employment providers to offer strong, unique care to HIV-affected and reentry communities. The program also makes system-wide changes to help better coordinate services for returning citizens living with HIV and AIDS.
“This initiative allows a collaborative community participatory taskforce to coordinate case management, employment and housing services and improve health outcomes by working at three levels: client, provider and systems,” said Cynthia Tucker, Vice President of Prevention and Community Partnerships at AFC and the project’s leader. She indicates the program is critical to combatting stigma, homophobia and racism while creating policies and structural interventions to improve health outcomes of this focus population. AFC has led the reentry corrections case management program since 1999; since Tucker began leading it in 2005, the program has helped over 1,500 people living with HIV leaving state prisons and jails get connected to medical care, a home if needed, and support systems to help them take care of their health.
Illinois’ adult correctional system has the country’s eighth-highest population of people in jail or prison or on probation or parole, totaling 215,100 people ages 18 or older as of Dec. 31, 2015 . Many of the communities most impacted by the criminal justice system are also most impacted by HIV, including Black and Latino gay and bi- men, Black women and transgender women of color. In 2015, an estimated 686 people in Illinois jails or prisons were living with HIV or had confirmed AIDS cases, making up 1.5% of the total custody population . The Cook County Jail alone releases approximately 600 people living with HIV annually, according to Dr. Chad Zawitz, Director of the Continuity of Care Clinics at the Cook County Jail and CORE Center. Once released, they face additional challenges — such as lack of economic resources; high rates of mental health disorders, trauma, and substance use/abuse; and the dual stigma of HIV and corrections involvement — that complicate their health, life stability, and successful reintegration into the community.
SSRP works at the client, provider and systems levels to ensure that people leaving jail or prison who are living with HIV maintain good health so they feel better and ultimately achieve an undetectable viral load, which would make them unable to pass HIV on sexually to others. SSRP builds on AFC’s Corrections Program, which is funded by the Illinois Department of Public Health. The program partners with Cermak Health Services/Cook County Jail, prison discharge planners in Cook and its surrounding counties, and two facilities in Cook County’s public health system — the Ruth M. Rothstein CORE Center and Austin CBC — to identify HIV-positive returning citizens prior to discharge or as soon as possible post-release. The Corrections Program uses a team of intensive Ryan White HIV/AIDS Program Corrections Case Managers to coordinate access to, monitor usage of, and track client outcomes across a range of medical/behavioral, housing, employment and other support services. SSRP will leverage this existing infrastructure while strengthening AFC’s partnership with Christian Community Health Center (CCHC), which provides primary care, housing and employment services to communities of color on Chicago’s far South Side; and establishing new collaborations with the AIDS Housing Constituency Group — Chicago’s planning group for provision of HUD/HOPWA transitional/permanent supportive housing and housing assistance — and the Illinois Department of Commerce Office of Employment & Training, which administers federal funding for employment readiness, job training and job placement opportunities from the Workforce Innovation & Opportunity Act.
 By Ashley Slupski
By Ashley Slupski
First of all, congratulations! You did it! You took the first of many steps to living your healthiest life by getting health care coverage (and avoiding a hefty tax penalty).
If you missed the Open Enrollment deadline, you may still be qualified for a Special Enrollment period because of a life change or a loss of insurance coverage. This year, a special enrollment period will be available to anyone who was auto-enrolled in a plan because their previous plan was discontinued – including many people living with HIV and receiving Ryan White benefits.
Here are some ways you can make your health care coverage work for you:
1. Make your first premium payment. Paying your premium affects when your coverage starts and if you don’t pay your premium on time, you might lose your coverage. If your plan is canceled, you’ll most likely not be able to re-enroll until next year’s open enrollment. If you’re having trouble affording your premiums because of a life change, you may qualify for Medicaid, and make sure you’re getting assistance from the AIDS Drug Assistance Program your premiums if you qualify.
2. Find a primary care provider and specialists. Be sure your providers are in-network with your new insurance plan. If you have questions about if a service or doctor is covered or in-network, call the phone number included on your insurance card. You may also want to identify hospitals and urgent care facilities that are nearby and in-network before you need access to emergency services. Otherwise, you could be forced to pay big medical bills because you went to an out-of-network facility.
3. Plan and budget. If your plan has deductibles, co-pays or co-insurance, out-of-pocket costs can start adding up. There is no reason you shouldn’t get care just because you’re afraid of costs. Reach out to us if you have concerns about paying for HIV-related medical expenses at 312-784-9060.
4. Check the drug formulary! New insurance coverage will include a formulary – the list of prescription drugs your health insurance will cover. If you have HIV drugs or other prescriptions you take regularly, make sure they are on your insurance formulary. If they are not on the formulary, you may still be able to have them covered, but there may be delays or extreme high out-of-pocket costs. Reach out to us at 312-784-9060 with your concerns about HIV drug coverage. If you’re taking Truvada for PrEP, the PrEP4Illinois program can help you afford the cost of the medication.
5. Don’t rely on the emergency room. Now that you’ve worked to get coverage, only rely on the emergency room for life-threatening or serious medical emergencies. Emergency rooms provide the most expensive care and you may be charged more if you do not have a true medical emergency. For routine or non-urgent health issues, visit your primary care provider or a non-urgent walk-in clinic.
6. Make your first appointment. Your primary care provider is an essential part of your care team. You want to develop a good relationship them to help you achieve your health goals. When scheduling your first appointment, ask:
- Is the provider taking new patients?
- Does your provider accept your insurance plan?
- Is your provider in your insurance network?
- How will you be billed for health services and what are your options for paying them?
- What information will you need to bring when you go in for your appointment?
The chart below tells you more about how to contact your primary care doctor depending on your kind of coverage.
| Original Medicaid |
Medicaid-Managed Care |
HMO | PPO or POS |
|---|---|---|---|
|
You should be able to contact any provider directly to see if they accept Medicaid. If you call a doctor and they say they don’t accept Medicaid, they may know where else you can go if you ask.
|
You can contact your Care Coordinator for a referral to a doctor that is in your network. | You should have picked a primary care doctor when you enrolled. If you don’t know who your PCP is, call the customer service number on the back of your card. | You should be able to contact any provider directly to see if they accept your insurance. You can also check with your insurance company to see what providers are “in-network” in your area. |
By Alaina Kennedy
The AIDS Foundation of Chicago (AFC) and Pride Action Tank (PAT) strongly condemns the announcement by the U.S. Department of Health and Human Services (HHS) the creation of the Conscience and Religious Freedom Division (CRFD) in the HHS Office for Civil Rights (OCR). The Trump administration and HHS announced the CRFD will be tasked with “restoring federal enforcement of our nation’s laws that protect the fundamental and unalienable rights of conscience and religious freedom.” To those that work and promote health equity we know this act is intended to roll back critical protections that ensured people living with and vulnerable to HIV, women, LGBTQ individuals and other marginalized populations could not be denied medical care.
For more information click on the following links:
AFC and PAT Statement
Link to HHS OCR Division of Conscience and Religious Freedom
Policy Statement: Discriminatory Laws and Policies Affecting Lesbian, Gay, Bisexual and Transgender Individuals and the HIV and STD Epidemics
Shutdown watch: House voted to pass continuing resolution.
The third and current continuing resolution (CR) for fiscal year 2018 year expires tonight, January 19, 2018, at midnight. The House passed the CR that would fund the government through February 16, 2018 with a vote of 230 to 197. The resolution includes six year funding for the Children’s Health Insurance Program (CHIP) but does not include protections for Deferred Action for Childhood Arrivals (DACA) recipients. The bill now moves to the Senate where Democrats have indicated that they will not support any legislative that does not include protections for DACA recipients. Senate Majority Leader Mitch McConnell (R) is preparing for the possibility of a government shutdown and sent GOP members an email imploring them to assign blame to Democrats should funding lapse.
Politico Article: Congress hurtles toward shutdown
Medicaid Work Requirements and 1115 Waivers
CMS released guidance inviting states to request work requirements in in their Medicaid programs. Shortly thereafter, CMS approved the first such waiver request to implement this policy in Kentucky. The Medicaid program is a critical source of health coverage for life-saving care and treatment for people living with HIV. A majority of Medicaid enrollees already either work or live in working families, and it is precisely because their health care needs are met by the Medicaid program that these individuals are able to be productive. Rather than improving health outcomes as CMS proposes, a work requirement as a condition of Medicaid eligibility will harm people living with HIV either by disrupting access to coverage and lifesaving treatment or eliminating health care coverage altogether.
Governor Rauner has come out in support of work requirements in Medicaid.
Chicago Tribune Article: Medicaid Work Requirements Illinois
Protect Our Care Illinois’ denounce CMS work requirements
AFC and Pride Action Tankstrongly condemn the announcement by the U.S. Department of Health and Human Services (HHS) to create the Conscience and Religious Freedom Division (CRFD) in the HHS Office for Civil Rights (OCR). The Trump administration and HHS announced the CRFD will be tasked with “restoring federal enforcement of our nation’s laws that protect the fundamental and unalienable rights of conscience and religious freedom.”
To those that work and promote health equity we know this act is intended to roll back critical protections that ensured people living with and vulnerable to HIV, women, LGBTQ individuals and other marginalized populations could not be denied medical care. The Conscience and Religious Freedom Division will now use federal dollars to shield providers who choose to discriminate, instead of prioritizing vulnerable patients and provide services to improve their health is counter to the mission of HHS, wasteful of scarce federal funds, and will result in delayed or lack of care for vulnerable individuals, threatening their health and lives.
We call on the Trump administration and HHS to reverse this decision immediately!
 By Raven Feagins
By Raven Feagins
Dec. 13, 2017 was a cold night on the west side of Chicago, but just over 30 community members from across the city made the trip to gather at Malcom X College for the first Getting to Zero Illinois town hall. Getting to Zero is a state-wide initiative that will end the HIV epidemic in Illinois by implementing a statewide plan that is informed by communities most affected by HIV. This first town hall was a crucial step in the process; participants met to learn more about the framework and to express their concerns, hopes and thoughts on what actions are needed in order to achieve the Getting to Zero goal. The meeting space was filled with a mix of emotions and expectations for the night, but, most of all, everyone was there to share their ideas and kick start the Getting to Zero process.
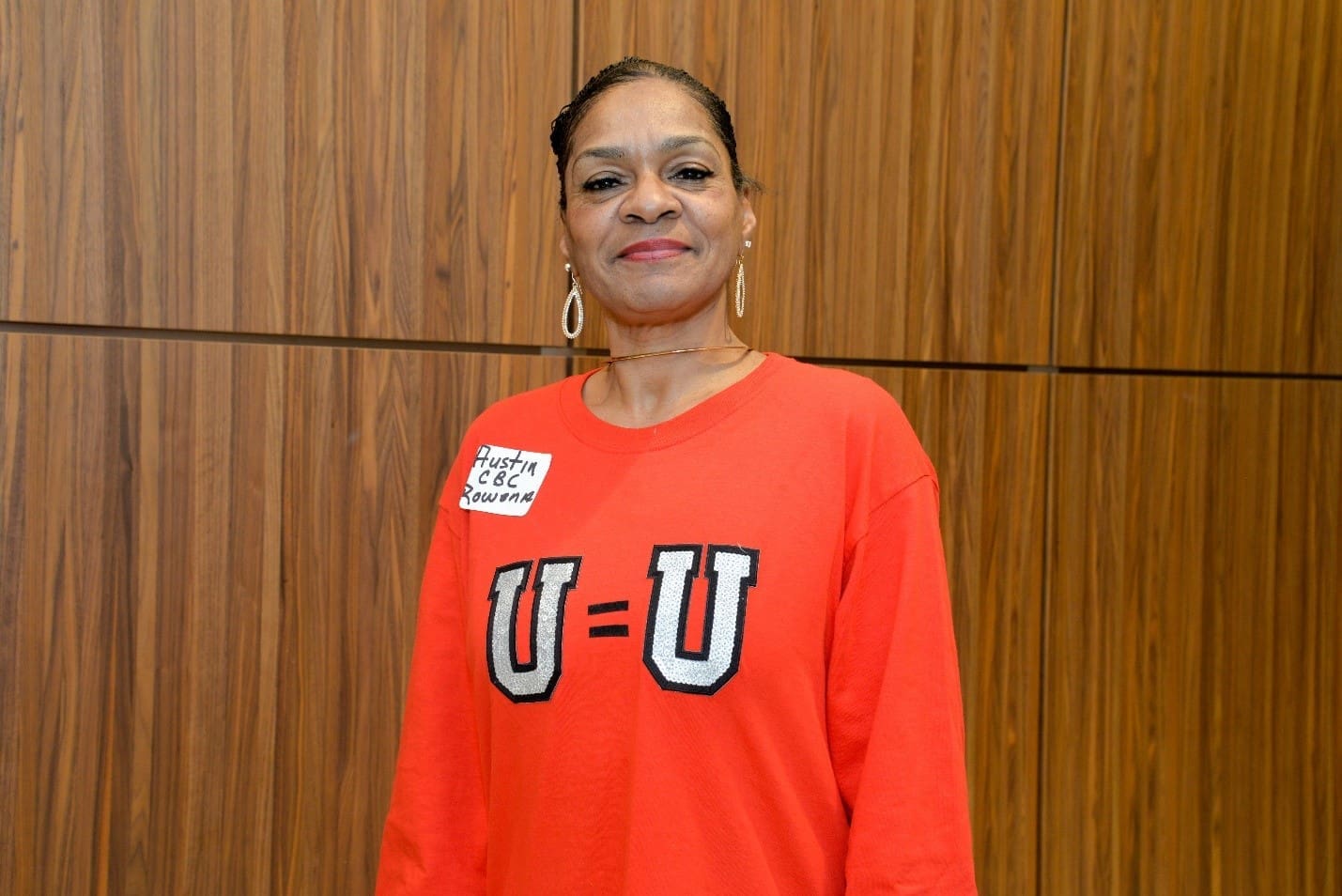
One of the most exuberant participants of the night was Rowena Thomas. Representing West Side health organization Austin CBC, she attended the town hall wearing a bright red shirt with the message “U=U” emblazoned on the front in bold, silver sequins. Thomas made it clear that her goal was to express the importance of having peer workers at hospitals and clinics across the state to share the insights they have gained through their experiences as people living with HIV. In her role as an HIV tester, Thomas has seen the positive impact of peer workers who help folks navigate their care options and support them in times of need. She believes investing in peer workers is essential to ending the HIV epidemic, and she was met with an applause of support after making the case to other town hall attendees. Overall, Thomas was energized by the meeting and thrilled to be part of the process that will benefit the communities she works with every day.
“I thought it was very exciting. I think that they need to do some more of these,” said Thomas. “It means that, you know, people are listening now.”
Aside from the importance of investing in peer workers, other common themes that came up throughout the night included: the need to first address various social determinants of health in communities heavily impacted by HIV, different solutions to tackle the stigma still attached to HIV and ensuring that medical providers are aware of and recommending new HIV prevention methods to patients, such as PrEP.
Community input is at the center of the Getting to Zero framework and the first step toward developing a solid plan. This was only the first of many town halls taking place across Illinois; head to gettingtozeroIL.org to RSVP for upcoming town halls in January 2018 and find out how you can get involved with Getting to Zero.
By Brian Solem
Housing and health are inseparably linked. You’re more likely to be in consistently good health if your housing costs (rent or mortgage plus utilities, groceries and other household needs) take up a limited slice (30% by most estimates) of your overall budget. If you are barely making ends meet, your health might show it, and you become more susceptible to unstable housing or homelessness.
Overall health is impacted by more than just your ability to receive health care,” said Jessie Beebe, Director of Behavioral Health for the AIDS Foundation of Chicago. “It’s all about the social determinants of health: environmental factors like a person’s living conditions, community, income, transportation options, education and more.”
A person’s economic situation can determine their physical and mental health — regardless of their race or ethnicity. A 2012 study in the International Journal of Health Services found that health disparities between people of different races were eclipsed by the disparities existing between high- and low-income groups within each racial/ethnic group. According to a Federal Reserve report on the economic wellbeing of U.S. households in 2016, 36% of respondents earning $40,000 or less went without some form of medical treatment. Only 23% of people with incomes between $40,000 and $100,000 and 9% of people making over $100,000 said the same thing. Housing isn’t the only reason someone might not get that cough or rash checked out, or refill their HIV meds before they run out, but it can have an impact.
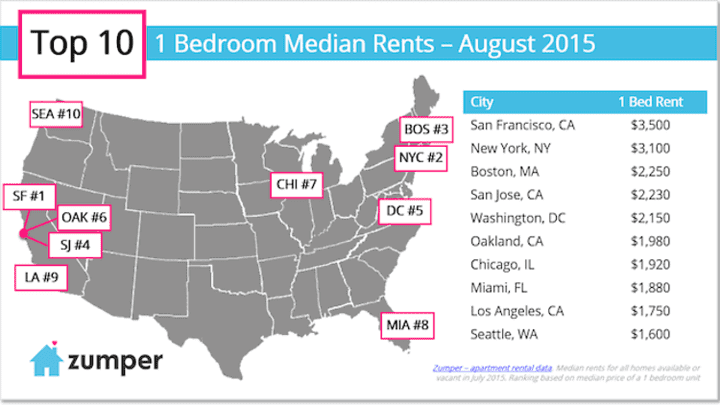
But what does income have to do with housing? Housing is the most fixed item in a person’s personal budget, which means it tends to get prioritized over all other recurring expenses that a person has to cover. Your rent and utility costs don’t typically change too much from month to month — but they do seem to be rising for most Americans, to the point that you need to make $21.21 per hour to rent a two-bedroom apartment (on average — this is much higher in big cities!). If your rent is significantly higher than you can “afford,” you’re not living with a cushion for health expenses.
Picture Rae — a fictional single mom with two children living in Chicago making just $10.75 per hour (the Chicago minimum wage) as a personal care aide. She’d have to work almost 80 hours a week to afford the average two-bedroom apartment in Illinois according to this study.
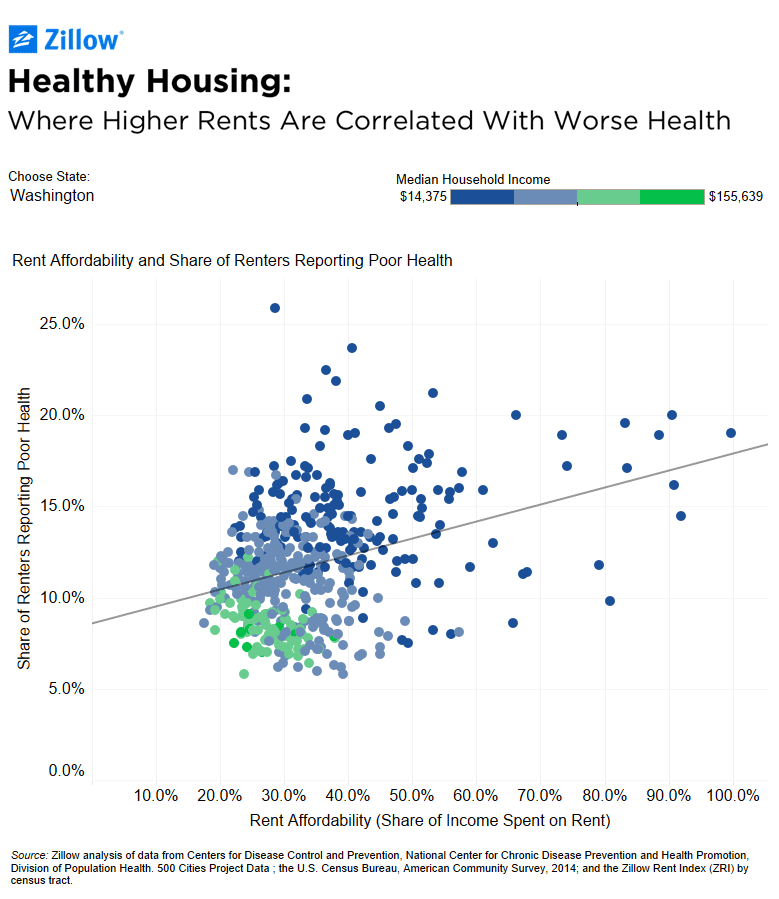
The message from our friends at Zillow is clear: if you can’t afford your rent, you’re very likely to also have poor health. If housing were more affordable, people could spend more on doctor visits, medicine and healthier food and lifestyle choices. But as long as housing costs continue to rise, people’s health will continue to decline. And if the Trump administration deprioritizes the needs of poor Americans and enact policies that actually increase housing costs, our health may experience a dramatic decline in 2018.
What’s the solution (besides burning capitalism to the ground and starting all over again)? Cities like New York, Los Angeles and San Francisco are making big moves to end homelessness and unstable housing by creating new homes for people who find themselves suddenly without housing. “Chicago just took a first step in the right direction by allocating $1.8 million in the calendar year 2018 city budget for a flexible rental subsidy pool targeted to homeless people with chronic illnesses.” Many people living at the edge of their budget who experience a sudden financial catastrophe like the loss of a job or a health crisis may find themselves without a home. Veronica, a real working mom from Chicago who needed emergency housing assistance from AFC to save her family from eviction after she and her husband became sick, is one such person.
“When you give a person a stable home, they can think about their health,” said Jessie. “They can have stability and safety that they didn’t have before, and then have space in their brain to worry about going to the doctor and taking good care of themselves.”
A home is reassurance. A home is strength and security. A home is a necessary ingredient in helping a person reach their full potential — in health and in life. Increasing wages, lowering housing costs and maintaining equitable approaches to providing health care for all (like the Affordable Care Act) can make a home possible for everyone.
Next steps:
What’s the real cost of living in your area? Find out using this Living Wage Calculator.
Sign up to take action with the National Low-Income Housing Coalition.
Learn more about social determinants of health through this interactive infographic.
Need a home or help keeping your home? Learn about housing programs offered by AFC and other organizations.
 By Will Wilson
By Will Wilson
Longtime HIV advocate and Chicago resident Will Wilson was invited to share his first-person account of using Medicaid and Affordable Care Act services to the people in charge of nationwide Medicare and Medicaid services.
It was cold, dark, and I was up way earlier than normal. Still, I was excited. I was heading to Washington D.C. to share my story with Calder Lynch, the Senior Counselor to the Centers for Medicare and Medicaid Services (CMS) Administrator Seema Verma. In other words, he’s the right-hand man to the person overseeing federal health insurance programs that many of us living with and vulnerable to HIV and other chronic conditions use to access health care thanks to the Affordable Care Act (ACA). I jumped at the chance to share my story because of the Trump administration’s threat to these essential programs.
We left Midway airport at 6 a.m. and returned eleven hours later – a one-day trip in the name of protecting health care access. We were part of a small group of HIV organizations from across the nation who have been advocating for sound Medicaid coverage for people living with and vulnerable to HIV including the Center for Health and Law Policy Innovation at Harvard Law School (CHIPLI), the HIV Medical Association (HIVMA) and the AIDS Institute (AI). Still, I was the star of the meeting to share my experience with these programs, because I’ve been enrolled in nearly all of them.
After brief introductions and the reasons for the meeting everyone’s attention turned in my direction. I shared with them how the health insurance I’d had when I was diagnosed turned out to be junk insurance and how paying for medications, lab work and doctor’s visits out of pocket landed me in medical bankruptcy. I told them how the Ryan White Care Act as well as the AIDS Drug Assistance Program (ADAP) helped me address my health issues before the ACA. I shared my frustration that both of these programs only deal with HIV and HIV-related issues. Like many others living with HIV I sometimes had other health issues to attend to that were either ignored or only taken care of when they could no longer be ignored.
I hoped I was smiling when I shared with Mr. Lynch the freedom I felt being able to enroll in the expanded Adult Medicaid program knowing that, for the first time since my diagnosis, I would have access to complete health care. I did my best to convey that my stress level decreased knowing I no longer had to worry about how to face any health challenge. I emphasized that if Medicaid were to disappear or Ryan White and ADAP programs became horrendously altered, I’d have some very difficult choices to make.
After I finished speaking, several specific policy issues were addressed and the meeting was concluded. Before we adjourned, Mr. Lynch spoke to me directly, looking me in the eye as he did. He thanked me for sharing my story. I felt in that moment that I’d actually been heard. He also said he’d be sharing his notes from this meeting with his boss, Seema Verma, the Administrator of the Centers for Medicare and Medicaid Services.
When I arrived home that cold December evening I wondered which of my small statements will have the most effect. While I’ve been a grassroots political advocate for HIV for only the past 15 years, I’ve been part of the HIV community from the very beginning, since before the virus had a name. In all this time I’ve seen more wonderful things than not. Advances in science allow us to live longer and healthier than ever before, and we’re getting closer to eradicating HIV, yet we still have quite a distance to cover. I’ll continue to focus on the positive while staying ever aware of the negative, pun intended.
Will Wilson seeks to serve those most in need as often as possible. He tested positive for HIV when the first tests came out in the 1980s. He chose to ignore the results until he was diagnosed with AIDS in May 2002.
Want to speak truth to power like Will? Join AFC’s Mobile Engagement Network and get updates on state and federal actions that affect health equity.
Or take your engagement one step further and join Illinois ASAP, a statewide coalition of HIV advocates. Contact Ramon Gardenhire at [email protected] for more info.