 The AIDS Foundation of Chicago (AFC) is pleased to announce that we were recently awarded a grant from ViiV Healthcare’s Positive Action for Women (PAFW) initiative. Continuing our dedication to supporting cisgender and transgender women of color, AFC will be partnering with Chicago Women’s AIDS Project, Affinity Community Services, Stroger Hospital and other Chicago leaders to develop and implement a local action plan to engage women in HIV prevention and care.
The AIDS Foundation of Chicago (AFC) is pleased to announce that we were recently awarded a grant from ViiV Healthcare’s Positive Action for Women (PAFW) initiative. Continuing our dedication to supporting cisgender and transgender women of color, AFC will be partnering with Chicago Women’s AIDS Project, Affinity Community Services, Stroger Hospital and other Chicago leaders to develop and implement a local action plan to engage women in HIV prevention and care.
“We’re going to build strategies that will change the political and environmental arenas for cis- and trans women of color,” said Cynthia Tucker, VP of Prevention and Community Partnerships for AFC. In addition to a career of work supporting women living with and vulnerable to HIV, Tucker is leading AFC’s Project Elevate campaign, which empowered young cis- and trans women of color to build a campaign and strategy to connect with young women in Chicago about HIV and STIs.
While the number of new HIV diagnoses among women of color declined from 2010-2014, of U.S. women newly diagnosed, 80% were U.S. women of color. Furthermore, complex social dynamics and isolation have limited the promise that medical advances could have in reducing the impact of the HIV epidemic. Responding to this situation, ViiV Healthcare is addressing the disproportionate impact of HIV among women of color in the U.S. through PAFW. PAFW is a pilot initiative that supports innovative, forward-thinking collaborations that break down isolation and stigma for cis- and transgender women of color living with HIV and link women to networks of care.
To learn more about this women-focused action plan, please contact Cynthia Tucker at [email protected]. For more information on PAFW and our co-grantees, visit the PAFW website here.

by Raven Feagins
Michelle Hennigan is a compassionate mother of one who lives in the small village of Johnsburg – just over an hour and a half outside of Chicago. Michelle loved providing a comfortable lifestyle for her and her daughter, but in 1999 – just as she was moving up in her career – Michelle became extremely ill with no sign of recovery.
“I was so sick at the time; I knew something was seriously wrong,” says Michelle. “I had gone to the emergency room a couple of times and, because I was working a couple of different jobs, I thought it was possibly stress-related. Then, they did some blood work, and the doctor said something about blood counts.”
Michelle’s experience in health care helped her realize that the doctor was referring to her T cell count – leading to the unsettling realization that she may be experiencing complications related to AIDS. She immediately told the doctors that she wanted to take an HIV test, and – just as she thought – the test came back positive.
“After the initial shock, I was kind of practical about it – I think I was a little bit detached. I was so sick and, being a single mom with a little one … I was just practical.”
Although Michelle physically felt better again, her mental health worsened as she sank into a deep depression. Michelle slowly become estranged from her close friends and family because of stigma against people living with HIV. Eventually, she struggled with a bad relationship with alcohol.
“I would kind of say it was like a tsunami. There’s one wave and then there’s another wave and another one. Just when you think you can come up for air and everything’s okay, you get hit again.”
Michelle was lonely. She didn’t have anyone to talk to about being newly diagnosed with HIV. The only referral she received after her diagnosis was to an infectious disease doctor. Michelle didn’t know where to turn for emotional or social support.
After receiving support to change her relationship with alcohol at a local church, Michelle decided it was time to find someone to support her with her new HIV diagnosis. She made phone calls to different organizations in the area, hoping someone on the other line will lead her in the right direction. One of those calls was to the AIDS Foundation of Chicago.
We connected Michelle to Open Door Health Center in Elgin, where she found helping relationships from support groups, therapy and her case manager, Sharon Marach. Michelle no longer felt like she was alone. Michelle found the resources she needs to flourish as a healthy, HIV-positive woman.
“She uses me more for resources,” Sharon said. “we also talk about things like what she wants to do in the future. Whatever she needs, I can provide it, and, if I can’t, I’ll find it.”
At AFC, we connect 159 case managers like Sharon with more than 6,000 people like Michelle every year. Together, they overcome health challenges, daily life struggles and so much more.
Now, the two of them are working out next steps for Michelle; she’s planning a move to Texas. Sharon is connecting Michelle to the HIV services there so she never feels alone again.
We receive calls like the one from Michelle on a daily basis. If you, or someone you know, needs help accessing HIV-related counseling, case management or other support services, give us a call at 312-922-2322 or send us a message at [email protected].
By Sara Semelka
 Illinois is making dramatic progress against HIV
Illinois is making dramatic progress against HIV
New HIV cases have dropped by 28% from 2006 to 2015. Mother-to-child HIV transmission is nearly eliminated. In Chicago, there were fewer than 1,000 cases a year. Because of this, it’s possible to end the HIV/AIDS epidemic in Illinois.
Illinois has what it takes.
With health care access expanded under the Affordable Care Act, powerful medications that stop people living with HIV from transmitting to others, and the HIV prevention pill PrEP, we can get to zero in our state.
But what does it mean
Getting to Zero means zero new HIV infections and zero people living with HIV who are not on treatment. Getting to Zero means getting more people in HIV treatment and getting more people to use the HIV prevention method that works for them.
Other places are having success.
We are inspired by efforts in New York, San Francisco and Washington state. Using what their experts learned, we created our own Getting to Zero Framework and a one-page 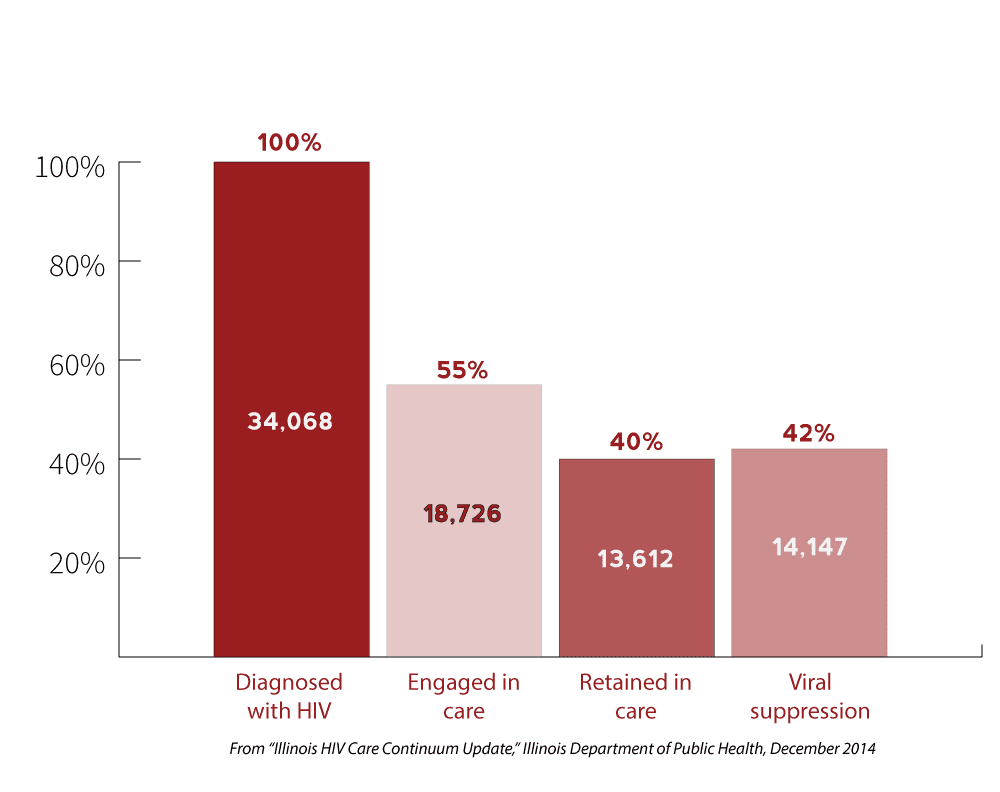 summary.
summary.
We need you to make it happen.
Now that we know we can get to zero, we need to figure out how, and that’s where you come in! Share your thoughts at upcoming town hall listening sessions and in an online survey. You’re a vital part of planning how Illinois will achieve zero new cases of HIV.
Stay tuned throughout the fall for announcements about our listening sessions and online survey, all of which will be posted on the GTZ web page.
The Getting to Zero steering committee includes representatives from the AIDS Foundation of Chicago, Alexian Brothers Housing and Health Alliance, Center on Halsted, Chicago Black Gay Men’s Caucus, Chicago Department of Public Health, Howard Brown Health, Illinois Department of Public Health, Illinois Public Health Association, Lake County Health Department, Northwestern University, Ruth M. Rothstein CORE Center and the University of Chicago.
 Although most universities and schools were closed in August, 11 public health professionals didn’t let that stop them from cultivating their skills and building networks. They attended the ninth annual Public Health Boot Camp, an intensive one-week educational program provided by the AIDS Foundation of Chicago (AFC) and the Institute of Public Health and Medicine (IPHAM), the nexus for all public health activities at Northwestern University’s Feinberg School of Medicine. The five-day-long program fast-tracks participants’ skills around HIV/AIDS and public health, leadership and career development and provides a platform for building professional connections with health professionals across Chicago.
Although most universities and schools were closed in August, 11 public health professionals didn’t let that stop them from cultivating their skills and building networks. They attended the ninth annual Public Health Boot Camp, an intensive one-week educational program provided by the AIDS Foundation of Chicago (AFC) and the Institute of Public Health and Medicine (IPHAM), the nexus for all public health activities at Northwestern University’s Feinberg School of Medicine. The five-day-long program fast-tracks participants’ skills around HIV/AIDS and public health, leadership and career development and provides a platform for building professional connections with health professionals across Chicago.
“HIV is still really new to the overall epidemiological world,” said Cynthia Tucker, vice president of prevention and community partnerships at AFC. “HIV professionals need to borrow lessons from people working on other public health challenges and build collaborations and partnerships. The Boot Camp is a great opportunity to do that.”
Leah C. Neubauer, Assistant Professor of Preventive Medicine, and Grisel Robles-Schrader, Research Portfolio Manager for Community & Stakeholder Engagement from the Center for Community Health, led the Northwestern efforts. Neubauer remarked, “It’s a great honor to work with the AIDS Foundation of Chicago, our Program in Public Health and Center for Community Health to develop and implement a public health training institute.” Robles-Schrader cited the “valuable opportunity to collaborate with AFC and faculty from across the country to work with participants to expand and enrich public health practice.”
Full days of workshops facilitated by public health leaders and academic researchers equip enrollees with the ground work of best practices in public health, which then they apply to capstone projects that they can take back to their organizations.
One such participant, Anthony Betori, used Public Health Boot Camp to further develop their plan to create accessible institutes for public health within communities. A former teacher, Betori fleshed out their plan with the oversight of Public Health Boot Camp leaders and suggestions from their cohort members.
“Public Health Boot Camp has directly improved my ability to better train people for entry-level positions in HIV prevention and care,” said Betori. “I will be taking things I learned … to improve my practice as an educator and strengthen the foundations of the Community Health Apprenticeship Program at Chicago House.”
 Seventy-five people have completed the program since its inception, all of whom still work within HIV and have experienced career growth. The Boot Camp often invites alums to teach sessions, like Johnathon Briggs, Senior Vice President, Digital at Chicago-based PR firm Public Communications Inc. He led a workshop around social marketing and its impact on public health behavior.
Seventy-five people have completed the program since its inception, all of whom still work within HIV and have experienced career growth. The Boot Camp often invites alums to teach sessions, like Johnathon Briggs, Senior Vice President, Digital at Chicago-based PR firm Public Communications Inc. He led a workshop around social marketing and its impact on public health behavior.
“I’ve been part of the HIV community as an activist, advocate and lobbyist since before the virus had a name, some thirty-odd years ago,” said Will Wilson, another participant and a member of AFC’s Illinois Alliance for Sound AIDS Policy (IL ASAP). “I’m grateful for the new tools I’ve learned and I plan to put some of them to use. More importantly, I’m grateful for the time I got to spend with future HIV community leaders.”
AFC and Northwestern University plan to release dates for the 2018 Public Health Boot Camp this fall; for the latest information, visit aidschicago.org/PHBC.
2017 Participants
- Eric Amaya, CALOR
- Tony Anderson, Chicago House
- Anthony Betori, Chicago House
- Sanford E. Gaylord, Regional Resource Network Program at the U.S. Department of Health and Human Services – Region V
- Jemeika M. Hicks, AIDS Foundation of Chicago
- Eduardo Mendoza, DePaul University
- Donna Sinclair
- Megan Sutherland, Children’s Place
- Will Wilson, IL ASAP
- Mara Williamson, AIDS Foundation of Chicago
- Thomas Zahorik, Dr. Jorge Prieto Family Health Center
Fourteen health and social justice organizations from across the U.S. wish to celebrate the people-powered effort behind UnitedHealthcare responding so swiftly to demands that they improve access to the HIV drug Truvada for pre-exposure prophylaxis (PrEP), a medical intervention that prevents HIV infection. On Friday, Aug. 4, UnitedHealthcare received a joint letter from this coalition objecting to new prior authorization rules put in place for access to PrEP effective July 1. These burdensome rules required patients to request access to PrEP every three months, denied claims for some based on highly offensive and discriminatory criteria, and forced UnitedHealthcare members to use the insurer’s mail-order pharmacy program to receive the medication. Within hours, UnitedHealthcare posted a public response to the groundswell of complaints against its PrEP policy. The insurer removed the prior authorization requirement for Truvada and now allows members on PrEP to fill their prescriptions at any UnitedHealthcare in-network pharmacy.
These organizations were not alone in this fight: Alongside their efforts to reverse UnitedHealthcare’s practices were other activists, including Thomas Cinganko, who initially shared his denial letter helping to galvanize critical attention and action on this issue, and ACT UP NYC member James Krellenstein, who gathered more than 3,000 signatures and submitted them to the New York State Health Commissioner regarding UnitedHealthcare’s discriminatory practices. Multiple activist news outlets and reporters also added fuel to the fire regarding UnitedHealthcare’s unjust practices and contributed to its ultimate reversal. This multi-tiered approach to moving the needle on patient access to PrEP benefited from support from the grassroots up.
This is not only a model of advocates’ work in uniting to effect change that benefits peoples’ lives; it’s also an example of how major companies can tune in to the needs of their consumers and evolve their practices to better serve their members. We are aware of other insurers requiring Prior Authorization for PrEP, and we call on them to immediately halt that practice. We commit to monitoring them and closely observing changes to practices around PrEP that they may undertake, so that those who are most vulnerable to HIV are able to protect themselves from transmission.
AIDS Foundation of Chicago
AIDS United
APLA Health
Association of Nurses in AIDS Care
HealthHIV
Human Rights Campaign
HIV Medicine Association
National Coalition for LGBT Health
National Alliance of State and Territorial AIDS Directors
New York City’s Lesbian, Gay, Bisexual & Transgender Community Center
Project Inform
The AIDS Institute
San Francisco AIDS Foundation
Treatment Action Group
The AIDS Foundation of Chicago and partners demand United Healthcare halt their practices and policies that discriminate against the LGBTQ community.
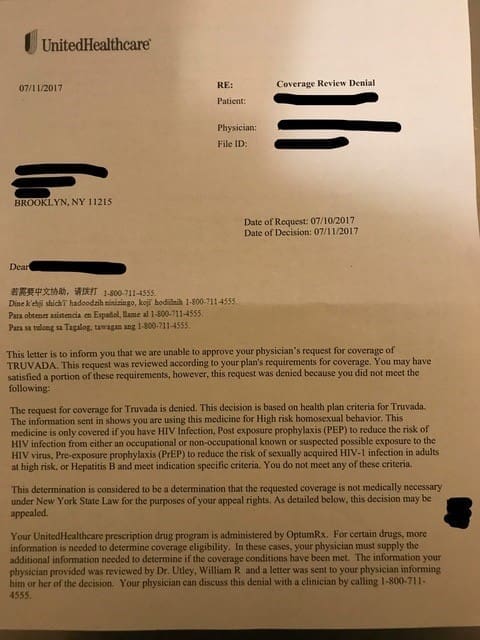
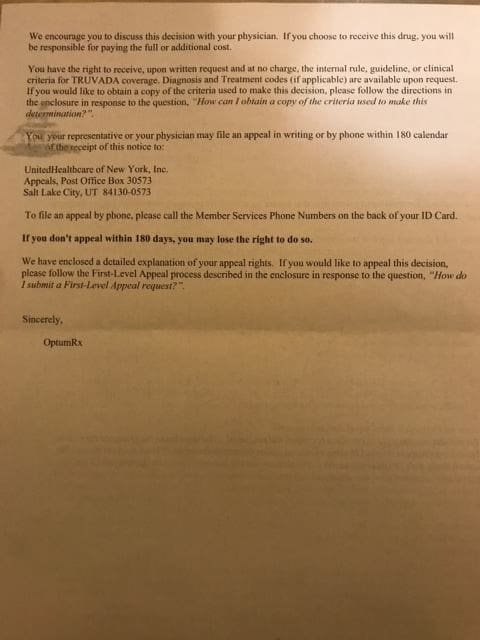
Earlier this year, United Health Care began to send members letters denying access to Truvada prescribed for Pre-Exposure Prophylaxis or PrEP. The reason for denial? According to the letter, shown in full below or click here to view, it was because the consumer was “taking this medication for High risk homosexual sexual behavior”. PrEP is a critical advancement in HIV prevention. UHC’s practices requiring members to receive PrEP through mail order pharmacies and denying PrEP without justification is not only discriminatory and dangerous – they are also illegal.
Read the full letter HIV advocates sent to UHC demanding they change their PrEP mandated prior approval process below.
Letter from United Healthcare Denying Access to PrEP
 |
 |
Letter from HIV Organizations to United Healthcare
August 4, 2017
Stephen J. Hemsley
Chief Executive Officer
David S. Wichmann
Office of the Chief Executive
President
UnitedHealth Group
P.O. Box 1459
Minneapolis, MN 55440-1459
Dear Mr. Hemsley and Mr. Wichmann:
We, the undersigned organizations, urge United Healthcare (UHC) to reverse the utilization management requirements that took effect July 1, 2017 for Truvada prescribed for Pre-Exposure Prophylaxis or PrEP.
Specifically, we believe requiring detailed documentation to request prior authorization every three months for Truvada prescribed for PrEP and requiring all members to use UHC’s mail-order pharmacy, BriovaRx, violates the Affordable Care Act (ACA)’s non-discrimination protections and federal and state laws barring mandatory mail order policies. We respectfully request a meeting to discuss the impact of these new policies on UHC customers.
PrEP is a critical advancement in HIV prevention that, when taken as prescribed, can provide nearly 100% protection from acquiring HIV infection. Stigma and discrimination are major barriers that have impeded uptake of this highly effective prevention intervention. In addition to violating multiple laws, the new policies have been implemented in such a way as to insult and disrespect UHC members. We have been shocked and appalled by the language in the coverage denial letters that are being sent to patients taking Truvada for PrEP and to patients living with HIV taking Truvada as part of a treatment regimen. The denials are contradictory and contain the type of inflammatory and judgmental language that contributes to the stigma that lesbian, gay, bisexual and transgender individuals and others face. In addition to written communications, UHC members have been subject to inappropriate and invasive questioning about their sexual orientation, HIV status and drug use by customer service representatives.
Excerpt from an OptumRx Denial letter:
“Your request for coverage for Truvada is denied. This decision is based on health plan criteria for Truvada. The information you sent in shows you are taking this medication for High risk homosexual sexual behavior. This medication is only covered if you have HIV Infection, Post exposure prophylaxis (PEP) to reduce the risk of acquisition from either an occupational or non-occupational known or suspected possible exposure to HIV, Pre-exposure prophylaxis (PrEP) to reduce the risk of sexually acquired HIV-1 infection in adults at high risk or Hepatitis B and meet indications specific criteria. You do not meet any of these criteria.”
We urge you to consider the points outlined below and immediately reverse the prior authorization restrictions implemented in July 2017.
UHC’s Policy Requiring Prior Authorization for PrEP Violates Non-discrimination Protections
The federal Medicaid Act and Section 1557 of the ACA prohibit discrimination on the basis of race, color, national origin, disability, age, and sex. Section §1557 prohibits insurance companies that participate in the state exchanges from discrimination based on these characteristics. The sex protections within the ACA have been interpreted to include gender identity, and sex stereotyping which many courts and federal agencies have implemented to also include sexual orientation. These protections extend to discriminatory drug benefit designs, including unjustified prior authorization processes. With specific regard to HIV medications, the court has ruled that placing arbitrary barriers on HIV medications constitutes discriminatory plan design. This applies to PrEP, which is primarily prescribed to gay, bisexual, or same-gender-loving men; black women; or transgender women.
UHC’s Prior Authorization Policy Is Restricting Access without Justification
We strongly object to the stringent and overly complex prior authorization documentation that is now required to request coverage of Truvada for PrEP. The medical providers prescribing PrEP are better positioned to determine the clinical appropriateness of PrEP for patients as evidenced by the communications that have occurred regarding this issue and the inappropriate denial letters UHC members have received. If prior authorization is maintained, we urge for the process to be significantly simplified and streamlined and for best practices to be followed. In particular, the approval period should be for 12 months, as is standard practice for medications that are prescribed for an extended period. The three-month cycle puts patients at risk of delays and medication interruptions and creates unnecessary burden to providers and anxiety for UHC members.
In order to protect against HIV acquisition, a patient must have consistent access to PrEP without interruption. Delays caused by UHC’s prior authorization approval put individuals at greater risk for acquiring HIV infection.
From a UHC Member:
“I have been on PrEP for three years and with UHC for the past year. I called in a refill of my Truvada to my local Walgreens on Saturday, July 1, with two pills left from my previous month’s prescription. I went to the Walgreens to pick up my prescription where I was told by the pharmacist that United Healthcare was requiring a prior authorization for my Truvada.
I called United Healthcare and they confirmed that a prior authorization was now required for Truvada and that a prior authorization request had already been sent to my doctor. I called the doctor’s office to find out if the prior authorization was approved. The office told me that the authorization was denied and I needed to call UHC to find out why. I then called UHC and asked if I could appeal the denial and I was told that I should call my doctor and have them call United Healthcare to start the appeal.
I called my doctor’s office and told them that I wanted to appeal the denial. The doctor’s office said that they need to ask me a few questions in order for the doctor to write a letter of appeal. I was asked how many men I have had sex with, was I a receptive anal sex partner, have a slept with HIV positive men, and if I had ever done crystal methamphetamine. I told the doctor’s office that I did not feel comfortable answering these questions.
I called United Healthcare and I asked to speak with a supervisor. The supervisor told me that it would take up to 15 days to do an appeal and five days to do a prior authorization once the HIV test was done. I told the supervisor that I was out of my Truvada prescription and I asked for them to cover a five day supply and they refused. I was also told that I would be required to fill my prescription through United Healthcare’s mail-order pharmacy.
This was an incredibly frustrating experience and I hope that United Healthcare addresses the barriers they created in having patients fill their Truvada prescriptions.”
UHC’s Mail Order Pharmacy Requirement Violates Existing Law
UHC is in violation of the ACA, 45 CFR § 156.122(e). The law requires any health plan required to offer Essential Health Benefits to allow enrollees to access prescription drug benefits at in-network retail pharmacies, unless there are specific safety or handling requirements that would preclude use of a retail pharmacy. Since July 1, UHC has repeatedly failed to provide an opt-out process for customers prescribed PrEP.
In addition to violating federal law, a number of states have statutes that bar mandatory usage of mail order. Georgia Code § 33-64-7-2, effective July 1, 2017, prohibits insurance companies that own pharmacy benefit managers from requiring their customers to use a mail order pharmacy. New York State’s Anti-Mandatory Mail Order Law similarly prohibits pharmacy benefit managers from requiring that patients purchase prescription drugs from a mail order pharmacy or pay an additional co-payment fee when such purchases are not made from a mail order pharmacy.
The mail order requirement is in violation of the 2014 Settlement Agreement arising from John Does I-V v. United Healthcare Insurance Company. The U.S. District Court of the Central District of California ordered United Healthcare to allow their customers taking HIV medications to opt-out of a mail order pharmacy requirement due to concerns about safety and privacy. The plaintiff class was concerned that their HIV status and sexual orientation would be inadvertently disclosed during delivery of their medications. UHC customers taking PrEP share those concerns.
Home delivery of medications to individuals in shared living situations or without secure mail receptacles puts UHC members living with stigmatized conditions or at risk for stigmatized conditions at unnecessary risk for stigma and discrimination. Truvada also is prescribed to treat HIV and discovery of the medication and other HIV medications threatens UHC members’ safety and privacy, potentially leaving them at risk for violence and discrimination.
From a UHC member:
“Since December 2015 I have picked up Truvada at a local retail pharmacy by opting-out of the mail-order requirement and having UHC grant an exception to deliver my meds to this specific pharmacy. Now due to the changes that went into effect 1 July 2017 (which I am still unsure what those changes are), the customer service representatives at UHC tell me that I can no longer opt-out. I repeatedly told them that I have major privacy and security concerns over receiving my PrEP through the mail, and they just now seem to be interested in looking to grant me another exception. I am out of PrEP as of tomorrow, and UHC will be responsible for this outrageous and unacceptable lapse in coverage. I am in school to become a physician and this process is mind-bendingly confusing even for me – I cannot fathom how someone without my level of health literacy could navigate these added barriers. This is an attempt to confuse and intimidate a vulnerable population into forgoing the lifesaving preventive services we deserve.”
Conclusion
In response to these concerns, we urge UHC to:
1. Remove the prior authorization requirement for Truvada for PrEP. If a prior authorization process is maintained, it should be significantly streamlined, invasive personal information should be removed, and be approved for a 12-month period.
2. Remove the mail-order pharmacy requirement and allow customers to opt-out.
PrEP is an effective prevention intervention that can help to stop HIV in its tracks. UHC members should not be denied access to this highly effective HIV prevention tool.
UHC’s prior authorization process is discriminatory and unnecessarily complicated, and the mail order requirement is illegal. For the reasons stated above we believe these actions are discriminatory in nature and reserve the right to pursue this matter further by filing a complaint with the U.S. Department of Health and Human Services Office for Civil Rights, charging unlawful discrimination under the Affordable Care Act’s non-discrimination protections.
We reiterate our request to meet with you immediately to discuss the UHC prior authorization policy for PrEP. We look forward to your response within 10 business days.
To schedule a meeting or to resolve questions regarding this letter, please contact:
Ramon Gardenhire, AIDS Foundation of Chicago, (312) 334-0928 or [email protected]
Benjamin Brooks, Health HIV, (202) 507-4737 or [email protected]
Respectfully,
AIDS Foundation of Chicago
AIDS United
APLA Health
Association of Nurses in AIDS Care
Health HIV
Human Rights Campaign
HIV Medicine Association
National Coalition for LGBT Health
National Alliance of State and Territorial AIDS Directors
New York City’s Lesbian, Gay, Bisexual & Transgender Community Center
Project Inform
The AIDS Institute
San Francisco AIDS Foundation
Treatment Action Group
by Raven Feagins
 Millions of people across the country are unable to work most jobs and earn an income due to disability or other challenges. For these folks, Supplemental Security Income (SSI) and Social Security Disability Insurance (SSDI) are available to help supplement, but the application process is known for being nearly impossible to navigate. This inspired the creation of the SOAR (SSI/SSDI Outreach, Access and Recovery) program, which the Center for Housing and Health, a supporting organization of the AIDS Foundation of Chicago, has since adopted to help support their clients.
Millions of people across the country are unable to work most jobs and earn an income due to disability or other challenges. For these folks, Supplemental Security Income (SSI) and Social Security Disability Insurance (SSDI) are available to help supplement, but the application process is known for being nearly impossible to navigate. This inspired the creation of the SOAR (SSI/SSDI Outreach, Access and Recovery) program, which the Center for Housing and Health, a supporting organization of the AIDS Foundation of Chicago, has since adopted to help support their clients.
The SOAR model involves training case managers to specifically assist people experiencing or at risk of homelessness who also have a mental illness, medical impairment, and/or a co-occurring substance use disorder. The program’s goal is to help these individuals successfully gain access to SSI and SSDI benefits. Since 2006, the SOAR program has helped with the success of over 31,000 application approvals nationwide, and Daniel Garcia, a 47 year-old Chicago native from the Humboldt Park neighborhood, is just one of the many people who have benefited.
Garcia, who possesses an exceptionally warm demeanor and walks with a slight limp, was exposed to drugs from an early age. He believes this led to the development of his addiction, which eventually took a serious toll on his body. The side effects of his repeated use caused his hip bones to start deteriorating, which made it painful for him to stay on his feet. He worked as a busboy at a downtown pizzeria when the pain became unbearable, and Garcia was forced to quit due to the nature of the work. Although he changed his relationship with drugs and was no longer using, the pain continued to intensify. He found himself without any source of income and limited options, so Garcia decided to apply for SSI benefits. While it was clear that he was unable to continue working, especially since doctors were recommending he get hip replacement surgery, his application was still denied. Garcia had nowhere to turn for support, and eventually found himself living on the streets.
“I lived for 6 or 7 months underneath the viaduct,” says Garcia. “I didn’t want to steal, so I asked for change … until my hips started getting worse. Then, I caught a case.”
Garcia was charged for retail theft and faced possible time in jail. However, the judge assigned to his case made the decision to, instead, send him to live at A Safe Haven, a social enterprise that focuses on helping improve the lives of those who seek assistance with health, education, housing and employment. Garcia repeatedly refers to this moment in his life as a blessing because it was here, at A Safe Haven, where he began to have a new outlook life.
“I came here and went to school; I took computer classes. Every time I went to court, [the judge] saw me and said, ‘You’re doing good,'” says Garcia. “That right there showed me that this is a second hint that God keeps giving me … to change and leave the old lifestyle alone.”
Things were looking up for him; Garcia was thriving in this new environment. He lived there for a total of six months, and made connections with several of the people who worked at A Safe Haven, including Jimia “Mia” Stokes, a case manager. Garcia gravitated towards Stokes who he found easy to talk to and someone who he could put his trust in. Stokes helped Garcia access a wide range of services, but one of the biggest things she did was help him continue his journey to receive SSI benefits by connecting him to the SOAR program at the Center for Housing and Health.
“Every time I went to court, [the judge] saw me and said, ‘You’re doing good,'” says Garcia. “That right there showed me that this is a second hint that God keeps giving me … to change and leave the old lifestyle alone.”
The Center focuses on connecting people to secure housing in order to better improve their health. In support of this mission, they recruited two full-time SOAR Specialists, Aaron Voldman and Lauren Rockoff.
“We work with people for five months or less, usually, and then we go through their paperwork,” says Rockoff. “We [pull all their medical records] to piece together any bits of the story. We make sure everything is consistent for Social Security so that they have the best possible chance to win their case.”
This was exactly the support and guidance that Garcia needed. He worked closely with Voldman during his application process and constantly felt reassured that, this time around, his application would be successful. Voldman helped Garcia understand the importance of building medi cal evidence for his application, and, soon enough, Garcia was the one taking control.
“Daniel took great responsibility for his own health care. He made and kept his own medical appointments and he got the treatment he need ed,” says Voldman. “The responsibility he took for his own wellness both benefited his health and created medical evidence necessary to win his disability income case.”
Soon after they met, Garcia went through with his first hip replacement surgery and moved out of A Safe Haven. Recovery from surgery often made it challenging to travel to medical appointments, but Voldman was always willing to help out. Whether it be finding him a ride or escorting him to an appointment, Garcia never felt alone.
“I got to know him as a friend,” says Garcia. “Everything he told me he was going to do, he did. He’s on his stuff!”
After about 5 or 6 months of the initial application submission, Garcia received the exciting news that he won his case and that he would soon start to receive his supplementary income. He is currently approved to receive up to three years of benefits, which is the same amount of time his doctor recommends he will need to fully recover from surgery. While the monthly amount for this type of benefit comes out to a national average of a modest $735, it’s enough for Garcia to get a start on his new chapter in life and live with a little more stability.
Garcia continues to frequent A Safe Haven for various classes, programming and to check in with Stokes. He is also in recovery from his second hip replacement surgery, and plans to study to become a counselor for young people who struggle with drug addiction in the Humboldt Park neighborhood.
Although he has been through a lot life-changing experiences over the past few years, Garcia managed to always embrace the supportive people who surround him. Looking back, he reflects on the support he received from people like Voldman and Stokes: “Having good people like Aaron or Mia … that shows me that there’s people that care … We come to these programs and think, ‘Oh, everybody’s here for their jobs.’ No, there’s people here that care.”
 AIDS Foundation of Chicago (AFC) strongly condemns the actions taken by a majority of Senate Republicans’ vote to advance a bill that would repeal the Affordable Care Act (ACA), which has provided access to comprehensive health care coverage for nearly 24 million Americans. If signed into law by President Trump without a proper replacement, over 1.2 million Illinoisans would lose their health care coverage, including 12,000 Illinois residents living with HIV.
AIDS Foundation of Chicago (AFC) strongly condemns the actions taken by a majority of Senate Republicans’ vote to advance a bill that would repeal the Affordable Care Act (ACA), which has provided access to comprehensive health care coverage for nearly 24 million Americans. If signed into law by President Trump without a proper replacement, over 1.2 million Illinoisans would lose their health care coverage, including 12,000 Illinois residents living with HIV.
The Senate’s actions yesterday place them one step closer to passing legislation that would wreak economic and medical havoc on millions of Illinoisans. The Congressional Budget Office (CBO) estimates a newly revised ACA replacement plan unveiled yesterday by Senate Republicans. Referred to as the “skinny bill,” it would increase the number of uninsured Americans by 15 to 30 million over the next ten years. A comprehensive draft of a replacement failed to pass in the Senate Tuesday night.
“It’s time for elected officials to remove themselves from the shadow of President Trump and stand up for every individual in their respective states, especially those with preexisting conditions,” said John Peller, president and CEO of the AIDS Foundation of Chicago. “Washington Republicans should not hide behind a façade of secrets and closed-door negotiations when discussing life-or-death legislation impacting millions of Americans. Tuesday’s vote corroborates that.”
In previous CBO and expert analyses of past failed Republican replacement plans, the funds promised to aid Americans living with preexisting conditions like HIV were appalling, stripping millions of individuals with pre-existing conditions of their health insurance.
The ACA dramatically increased health insurance coverage for people living with HIV in Illinois. As of 2016, at least 12,000 people living with HIV in Illinois recently gained health care coverage through the ACA, which is roughly 32 percent of people with HIV in Illinois, or 1 in 3 of the 37,788 reported Illinoisans living with HIV (IDPH, 2016).
Medicaid is an essential source of care for 55 percent of Illinoisans living with HIV (20,782 people in 2016). Repealing the ACA will result in vulnerable individuals losing or facing challenges when accessing care.
“We thank both Illinois Senators Richard Durbin (D-IL) and Tammy Duckworth (D-IL) for their examples of courage and voting against yesterday’s Motion to Proceed,” said Ramon Gardenhire, vice president of policy and advocacy for the AIDS Foundation of Chicago. “They continue to stand strong for people living with and vulnerable to HIV and all Illinois families.”
The fight continues and AFC, along with thousands of our allies and partners nationwide, will continue advocating for the health and welfare of all Americans. AFC urges Illinoisans and the American constituency alike to call Congressional leaders and demand that the repeal of the ACA not be carried out without a proper replacement. AFC stands ready to work with Members of Congress to develop a bipartisan plan that accounts for all the health care needs of Americans, including those living with and vulnerable to HIV.
by Ashley Brown
UPDATE: In November 2018, the Illinois Department of Health and Family Services (HFS) announced that a hepatitis C cure would be accessible for thousands more Illinoisans on Medicaid, many of whom were previously denied treatment until they reached end-stage disease. Learn more here.
Peter McLoyd doesn’t care what you think of him. From addiction to advocacy, his story has been defined by overcoming obstacles. From substance abuse to stigma to health inequity, McLoyd has seen it all. At 64, his long and winding road has led him to his current role as the Consumer Development and Advocacy Coordinator at the Ruth M. Rothstein CORE Center, which treats HIV, hepatitis C (HCV) and other infectious diseases.
McLoyd recently sat with AFC staff in his office on a sunny day in June, recalling his past struggles with drug addiction, as well as challenges navigating the health system as someone who is HIV-positive and as someone previously living with HCV. Soft-spoken and well-dressed, McLoyd is honest about himself and the winding road he has taken to where he is today. 
Speaking with a slight twang he developed from a childhood in the South, McLoyd traced his migration to Chicago, where his family moved to better care for his childhood illnesses. The trauma of uprooting his life to a new and foreign city, coupled with other childhood experiences followed McLoyd throughout his youth, until he started experimenting with drugs in high school. By senior year, he was injecting heroin and using cocaine, a practice that continued into adulthood.
Despite his struggles with addiction, McLoyd married and had children, and began work as a steel worker. A workplace injury led to a hospital stay that would impact his life for decades. Before surgery, a nurse entered his room to tell him of abnormal lab work they had discovered.
“I can remember that so clearly, forty years later,” McLoyd recalls. “She said it was hepatitis, ‘There’s no treatment for it and there’s not much we can really do about it, but we want to let you know.’ And that was it. That was how I found out about hepatitis.”
With no treatment and no further education about his condition, McLoyd left the hospital and descended into deeper struggles with substance use. As addiction started to unravel his life, including his marriage and career, McLoyd’s health began unraveling as well. Suddenly plagued with mysterious ailments, including bronchitis, night sweats and sudden weight loss, McLoyd went to numerous ERs looking for answers. Finally in 1995, a doctor suggested his symptoms could indicate an HIV infection and suggested he get tested — but provided no resources on how or where.
Years later, McLoyd is honest about his reaction to the news. “I was disturbed,” he recalls. “But I wasn’t surprised because I knew how HIV was transmitted, and I knew that I had shared needles.”
He struggled with the possibility and considered if he really wanted to know the truth. Even if he was living with HIV, treatment wasn’t widely available and an indifferent health care system gave him no further direction on testing or treatment, just as it had failed him with his diagnosis of hepatitis years before.
“It was a little anger at the fact that they were telling me that I might have an infection that could lead to death and just telling me to find a place to get tested,” McLoyd says.
So he left the hospital, unsure of his HIV status. But chance had other plans for McLoyd and his future. Within the next year, he found himself in jail, where he found a magazine article on Dr. David Ho and his work with HIV-positive injection drug users in New York City.
“That article just really resonated with me,” he remembers. “He was talking about African-American men who were injectors, and I could see myself in that group.”
With newfound hope, McLoyd committed himself to get tested. When he was finally tested in 1997, his illness had progressed to a point where he was wasting to nothing, weighing only 130 pounds and suffering from pneumonia, thrush and numerous other infections. McLoyd found his way to the hospital and toward a new life of health and possibility, since by that time, powerful new HIV treatments were available.
As McLoyd recovered, he realized the full impact of his addiction on his life and well-being.
“Because of my addiction, I hadn’t even noticed that I was basically skin and bones,” he remembers. “In order to deal with my HIV and become the person who I had strived to be as a young man and make a difference in the lives of other people, I had to let the drugs go.”
“I wondered how many other people were like that, who were just kind of left to their own devices and probably didn’t make it,”
With the help of therapy and peer educators, McLoyd began to address his struggles with substance use and began proper treatment for his HIV. As he dove into his new life with strength and resilience, McLoyd began to help others treat their addictions and improve their health, and he went from being a participant in the CORE Center’s peer educator program to managing it. From there, he became increasingly involved in HIV advocacy and policy, leading to his current role at the CORE Center.
Reflecting on his own recovery, McLoyd emphasized the importance of role models and representation in the treatment and recovery process.
“I had these role models, I could look at those people and say ‘wow, look at him, look at her, they did this, they can do this.’ Being encouraged and motivated by that was huge for me,” he remembers.
Tacking the hurdle of hepatitis C
It was also due to his involvement with the CORE Center that he finally received treatment for HCV. But as with other aspects of his life, it was not an easy road. As medications emerged to treat what McLoyd now understood to be hepatitis C, he began his first treatment of interferon and ribavirin therapy.
Despite warnings about the severity of the side effects, McLoyd thought he could handle it. After all, he was successfully maintaining his HIV and had overcome addiction. But right away, as McLoyd admitted, the treatment for HCV was a different ballgame than taking his HIV medications. Between pills and injections, he would be knocked out for days, with exhaustion and depression plaguing his body and mind. He made it through treatment largely with the support help of his new wife Kathy, but despite her loving support and the care of his physicians, the demanding treatment failed and did not cure his HCV.
Despite this, he remained hopeful. His optimism followed him into another failed year of HCV treatment, which initially showed promise, but ultimately did not clear his infection. Finally, in 2016, he began another year-length treatment with the new medication Harvoni, and the third time was the charm. Thanks to his upbeat nature and resilience, McLoyd can now say that after forty years and three rounds of treatment, his HCV has been cured. “It’s been a journey,” McLoyd acknowledges.
As McLoyd reflects on the long hard road he’s traveled to get to where he is today, he can’t help but consider the failings of the health system with his own conditions and wonder who fell through the cracks.
“I wondered how many other people were like that, who were just kind of left to their own devices and probably didn’t make it,” he considered.
But despite progress, McLoyd acknowledges the painful reality of health inequity today, especially among people living with HIV and HCV, and the power of pharmaceutical companies and the government in controlling care for those most in need.
 Treatment for HCV can cost upwards of $100,000 and Medicaid programs often deny treatment until the final, most severe stages of infection, when patients’ livers near failure and their health teeters precariously. Though steps have been taken in Illinois Medicaid to expand treatment to those with stage-three infections, thanks to AFC’s advocacy team and others, it is not enough. Such policies put patients in a vicious circle. They must be severely sick to get treatment, but will only get to the last stages of infection without the treatment. In the meantime, physicians tell them to care for their health to ensure they do not reach the last levels of infection that would make them eligible for treatment.
Treatment for HCV can cost upwards of $100,000 and Medicaid programs often deny treatment until the final, most severe stages of infection, when patients’ livers near failure and their health teeters precariously. Though steps have been taken in Illinois Medicaid to expand treatment to those with stage-three infections, thanks to AFC’s advocacy team and others, it is not enough. Such policies put patients in a vicious circle. They must be severely sick to get treatment, but will only get to the last stages of infection without the treatment. In the meantime, physicians tell them to care for their health to ensure they do not reach the last levels of infection that would make them eligible for treatment.
“There’s so much work to be done,” McLoyd confirms gravely, as he acknowledges the pain and frustration patients feel as they see others getting treatment, while being denied care.
“When you see other people getting treated and you’re not being treated, it’s just another way the world has rejected you; it’s very hard on the spirit,” McLoyd says. “It’s difficult to give people hope.”
HCV treatment is particularly important for those also living with HIV. Nearly one-quarter of people living with HIV in the U.S. are co-infected with HCV, and 50–90% of HIV-infected injection drug users also have HCV. Living with both HIV and HCV more than triples the risk for liver disease or liver-related death, and coinfection allows the disease to progress more rapidly. While AFC is working to end HCV transmissions in Illinois, and assist those living with HCV through the HCV Elimination Task Force, there is more work to be done for those living with HCV in Illinois.
Despite this, McLoyd is hopeful for the future of HIV and HCV treatment and the possibility of many diverse voices coming together to demand change. He particularly hopes his status as a heterosexual Black man and as a former injection drug user can influence the discussion around HIV and HCV treatment and prevention and lessen the stigma, particularly among heterosexual Black men. The power of representation of Black men struggling with addiction and an HIV diagnosis, from the magazine article to the peer educator program, encouraged McLoyd to transform his life and become the man and voice for change he knew he could be.
“As these efforts to end AIDS continue, my hope is that all voices will rise to the top to provide input and direction on what it requires to end AIDS in our communities,” he says. “We’re all in this together.”
By Raven Feagins
“Our Girls Matter.” That’s the tagline for the AIDS Foundation of Chicago (AFC)’s Project Elevate. The marketing pieces — developed for young cisgender (cis) and transgender (trans) women of color, by young cisgender and transgender women of color — feature photos of young women, with inviting, smiling faces that evoke a sense of community and needed action. The social marketing campaign, combined with other promotional materials, are sprinkled throughout AFC’s office and partner sites to encourage young Black and Latinx women to get tested for STIs and take control of their sexual health. 
Project Elevate is a three-year project funded though the CDC Community Approaches to Reducing Sexually Transmitted Diseases (CARS) initiative, and the women pictured are part of the project’s Youth Expert Advisory Board (YEAB). The board meets once a month and strategizes ways to mobilize more cisgender and transgender women of color to get tested for STIs, while also increasing awareness around common structural issues perpetuating STI disparities in the community.
But the work doesn’t stop at awareness-raising: Another key component of Project Elevate is the four-site STI and HIV testing network located at Lurie Children’s Hospital’s Center for Gender, Sexuality and HIV Prevention in Uptown and at Planned Parenthood’s Englewood, Austin and Roseland locations. As YEAB members focus on spreading awareness through outreach, events, attending conferences and community-building, these four testing sites serve as home bases for young cis and trans women of color seeking access to safe, culturally sensitive and culturally appropriate services.
Sheila Mahon is a big contributor to the work being done to create these safer and culturally sensitive services; she’s a Behavioral Research Associate at Lurie Children’s Center for Gender, Sexuality and HIV Prevention. Mahon runs the site’s Project Elevate testing, which involves speaking one-on-one with young participants in order to help them better understand sexual health, while also learning more about their experiences at the testing sites.
“I’ve seen [participants] from all over the city,” says Mahon. “A lot of the participants have told me, ‘Oh, I’ve been around the city and there aren’t many places to come in.’ … A lot of young women, they felt really comfortable [at Lurie] because it’s a safe space for them.”
The Lurie testing site is not a typical clinic. They have candy dishes full of condoms, free snacks and other donated materials for participants to enjoy. This setup helps make the environment a lot more inviting and welcoming for participants, while also addressing some of the other obstacles that participants might face.
Based on conversations with her participants, Mahon notices that there is a lack of sexual health information for women, likely related to inadequate sex education in schools and an absence of spaces for young people to discuss sexual health in a comfortable environment. She says, “[A] few of my participants had no idea what PrEP was, or any idea of how gonorrhea and chlamydia were transmitted. To talk to them about the raw details, instead of it being sugar-coated, is really important.”
Inadequate sex education in schools is a major problem across the U.S. and one of many structural issues that Project Elevate has identified that perpetuates STI disparities among young women of color. According to the U.S. Centers for Disease Control and Prevention (CDC), young women aged 15-24 experience disproportionately high rates of STIs and HIV throughout the country, with Black and Latinx women seeing disproportionately higher rates than white women. In Chicago, youth aged 20-29 made up 51.5% of all gonorrhea cases in 2015, and combined with youth aged 13-19, they represented 76.2% of all newly diagnosed cases of gonorrhea that year in Chicago. Furthermore, non-Hispanic Black populations were the most frequently diagnosed with new cases of HIV (54.1%), chlamydia (47.9%) and other STIs in Chicago, while Hispanic populations were also experiencing disproportionate rates of STIs. These numbers are already troublesome, but even yet, they still neglect to properly reflect the number of young, trans-identified women who are also disproportionately affected by high HIV and STI rates.
“A lot of the participants have told me, ‘Oh, I’ve been around the city and there aren’t many places to come in.’… A lot of young women, they felt really comfortable because it’s a safe space for them.”
Project Elevate has set out to reduce STI numbers and eliminate barriers to health care through their work. From October 2015 to June 2017, Project Elevate’s partner testing sites have administered 539 STI and HIV tests for young cis and trans women of color between the ages of 13 – 24 across Chicago. To get to the heart of systemic barriers that stand in the way of young women of color and health equity, L’Oreal Bailey, Project Manager of Special Projects at AFC, built a questionnaire and studies the resulting data to help identify those barriers within communities. The questionnaire asks about basic demographic information, such as age, ethnicity and race, while also asking questions regarding the participants’ living situations, whether or not they have heard of PrEP, and much more. The questionnaire is used to assess the work being done at testing sites, in case adjustments are needed to make them more accessible to the communities that Project Elevate prioritizes. For instance, Bailey notes that “At Planned Parenthood, we still have not seen any trans women of being tested, so that’s one of our challenges that we’re trying to kink out.”
 Bailey also works closely with YEAB members and notes how the testing program acts a useful tool for the members to continue their outreach and community building efforts. Her hope for the project is to be able to expand and connect with more young people and do more to support the YEAB members themselves.
Bailey also works closely with YEAB members and notes how the testing program acts a useful tool for the members to continue their outreach and community building efforts. Her hope for the project is to be able to expand and connect with more young people and do more to support the YEAB members themselves.
“They’re more than testing,” says Bailey. “We’ve all developed relationships with [YEAB members], but it’d be great to give them something in return … I want them to get more professional development skills as well as be able to give job placements for those members that need it.”
Project Elevate is an extremely unique and progressive initiative that strives to make sexual health accessible, safe and comprehensive for all young women of color. Although 2017 is the last year of the CARS grant for Project Elevate, there is still a lot of work to be done in order to combat the STI and HIV disparities in communities of color. Fortunately, Project Elevate has set the groundwork to continue mobilizing, engaging and centering the voices and experiences of young cis and trans women of color.